
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Copyright Notice
Licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Bookshelf ID: NBK596741

An official website of the United States government

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Open Resources for Nursing (Open RN); Ernstmeyer K, Christman E, editors. Nursing Skills [Internet]. 2nd edition. Eau Claire (WI): Chippewa Valley Technical College; 2023.
• Administer enteral nutrition
• Perform irrigation and suctioning of enteral tubes
• Select appropriate equipment
• Explain the procedure to the patient
• Assess tube placement
• Implement measures to prevent displacement of tube
• Modify procedures to reflect variations across the life span
• Document actions and observations
• Recognize and report significant deviations from norms
Enteral tubes are tubes placed in the gastrointestinal tract. Enteral tubes are used as an alternate route for feeding and medication administration, as well as for stomach decompression. Stomach decompression is a medical term that refers to removing stomach contents by using suctioning. Stomach decompression is commonly used after surgery or trauma to reduce pressure from fluids and gas that cause pain, nausea, vomiting, and potential aspiration of stomach contents into the lungs.
The nurse’s responsibilities when caring for a patient with an enteral tube include the following:
Administering enteral medication is discussed in “Administration of Enteral Medications.” The remaining responsibilities related to maintaining enteral tubes will be discussed in this chapter.
It is important to understand the anatomy and functioning of the gastrointestinal system before administering feedings or medications through an enteral tube. See Figure 17.1[1] for an illustration of the anatomy of the gastrointestinal system.

Anatomy of the Gastrointestinal System
Enteral nutrition is indicated for patients who need nutritional supplementation and have a functioning gastrointestinal tract, but cannot swallow food safely. Feedings can be administered via enteral tubes placed into the stomach or into the small intestine (usually the jejunum). For example, enteral feeding is commonly used for patients with the following conditions:
For short-term feeding, NG tubes are used. If the duration of feeding is longer than four weeks or if access through the nose is contraindicated, a surgery is performed to place the tube directly through the gastrointestinal wall (for example, PEG or PEJ tubes).
Patients who are not candidates for enteral nutrition are prescribed parenteral nutrition. Parenteral nutrition is a concentrated intravenous solution containing glucose, amino acids, minerals, electrolytes, and vitamins. A lipid solution is typically administered as a separate infusion. This combination of solutions is called total parenteral nutrition because it supplies complete nutritional support. Parenteral nutrition is administered via a large central intravenous line, typically the subclavian or internal jugular vein, because it is irritating to the blood vessels.
There are several different types of enteral tubes based on their location in the gastrointestinal system, as well as their function. Three commonly used enteral tubes are the nasogastric tube, the percutaneous endoscopic gastrostomy (PEG) tube, and the percutaneous endoscopic jejunostomy (PEJ) tube. See Figure 17.2[3] for an illustration of common enteral tubes. NG tubes are typically used for a short period of time (less than four weeks), whereas PEG and PEJ tubes are inserted for long-term enteral nutrition. Some institutions also place nasoduodenal (ND) tubes to provide long-term enteral nutrition. [4]

Types and Placement of Enteral Tubes
A nasogastric (NG) tube is a single- or double-lumen tube that is inserted into the nasopharynx through the esophagus and into the stomach. NG tubes can be used for feeding, medication administration, and suctioning. NG tubes used for feeding and medication administration are small and flexible, whereas NG tubes used for suctioning are larger and more rigid. NG tubes are secured externally on the patient’s nose or cheek by adhesive tape or a fixation device, so this area should be assessed daily for signs of pressure damage. See Figure 17.3[5] for an image of a small bore feeding tube.

Small Bore NG Tube
An example of a large bore nasogastric tube is the Salem Sump. Large bore nasogastric tubes, such as the Salem Sump, are used for gastric decompression. The Salem Sump has a double lumen that includes a venting system. One lumen is used to empty the stomach, and the other lumen is used to provide a continuous flow of air. The continuous flow of air reduces negative pressure and prevents gastric mucosa from being drawn into the catheter, which causes mucosal damage. This terminal end also has an anti-reflux valve to prevent gastric secretions from traveling through the wrong lumen. See Figure 17.4[6] for an example of a double-lumen enteral tube.

Double-Lumen Enteral Tube
Other types of tubes are placed through the patient’s abdominal wall and are used for long-term enteral feeding. A percutaneous endoscopic gastrostomy (PEG) tube is placed via an endoscopic procedure into the stomach. Alternatively, a percutaneous endoscopic jejunostomy (PEJ) tube is placed in the jejunum of the small intestine for patients who cannot tolerate the administration of enteral formula or medications into the stomach due to medical conditions such as delayed gastric emptying. See Figure 17.5[7] for an image of a PEG tube insertion kit and the appearance of an enteral tube as it exits from a patient’s abdomen.

PEG Tube
Feedings or medications administered into an incorrectly placed enteral tube result in life-threatening aspiration pneumonia. The placement of an enteral tube is immediately verified after insertion by an X-ray to ensure it has not been inadvertently placed into the trachea and down into the bronchi. See Figure 17.6[8] for an image of an X-ray demonstrating correct placement of an enteral tube in the stomach as indicated by the lower red arrow. (This X-ray also demonstrates an endotracheal tube correctly placed in the trachea as indicated by the top arrow.) After X-ray verification, the tube should be marked with adhesive tape and/or a permanent marker to indicate the point on the tube where the feeding tube enters the nares or penetrates the abdominal wall. This number on the tube at the entry point should be documented in the medical record and communicated during handoff reports. At the start of every shift, nurses evaluate if the incremental marking or external tube length has changed. If a change is observed, bedside tests such as visualization or pH testing of tube aspirate can help determine if the tube has become dislocated. If in doubt, a radiograph should be obtained to determine tube location. [9]

Placement Verification by X-Ray
After the initial verification of tube placement by X-ray, it is possible for the tube to migrate out of position due to the patient coughing, vomiting, and moving. For this reason, the nurse must routinely check tube placement before every use. The American Association of Critical‐Care Nursing recommends that the position of a feeding tube should be checked and documented every four hours and prior to the administration of enteral feedings and medications by measuring the visible tube length and comparing it to the length documented during X-ray verification.[10],[11],[12]
Older methods of checking tube placement included observing aspirated GI contents or the administration of air with a syringe while auscultating (commonly referred to as the “whoosh test”). However, research has determined these methods are unreliable and should no longer be used to verify placement.[13],[14]
Checking the pH of aspirated gastric contents is an alternative method to verify placement that may be used in some agencies. Gastric aspirate should have a pH of less than or equal to 5.5 using pH indicator paper that is marked for use with human aspirate. However, caution should be used with this method because enteral formula and some medications alter the gastric pH.[15]
Follow agency policy for assessing and documenting tube placement. Additionally, if the patient develops respiratory symptoms that indicate potential aspiration, immediately notify the provider and withhold enteral feedings and medications until the placement is verified.
The area of tube insertion should be assessed daily for signs of pressure damage. For NG tubes, the adhesive used to secure the tube can be irritating and cause skin breakdown. PEG and PEJ tubes may have fluid seepage around the insertion point that can cause skin breakdown if not cleaned regularly. Follow agency policy for cleansing the external insertion site for PEG and PEJ tubes. Cleansing is typically performed using gauze moistened with water or saline and then allowed to air dry before the fixation plate is repositioned. Because skin surrounding the insertion site is prone to breakdown, barrier cream or dressings may be prescribed to prevent breakdown.[16],[17]
Enteral Nutrition (EN) refers to nutrition provided directly into the gastrointestinal (GI) tract through an enteral tube that bypasses the oral cavity. Each year in the United States, over 250,000 hospitalized patients from infants to older adults receive EN. It is also used widely in rehabilitation, long‐term care, and home settings. EN requires a multidisciplinary team approach, including a registered dietician, health care provider, pharmacist, and bedside nurses. The registered dietician performs a nutrition assessment and determines what type of enteral nutrition is appropriate to promote improved patient outcomes. The health care provider writes the order for the enteral nutrition. Prescriptions for enteral nutrition should be reviewed by the nurse for the following components: type of enteral nutrition formula, amount and frequency of free water flushes, route of administration, administration method, and rate. Any concerns about the components of the prescription should be verified with the provider before tube feeding is administered.[18]
Tube feeding can be administered using gravity to provide a bolus feeding or via a pump to provide continuous or intermittent feeding. Feedings via a pump are set up in mL/hr, with the rate prescribed by the health care provider. See Figure 17.7[19] for an image of an enteral tube feeding pump and the associated tubing. Note that tubing used for enteral feeding is indicated by specific colors (such as purple in Figure 17.7). A global safety initiative, referred to as “EnFit,” is in progress to ensure all devices used with enteral feeding, such as extension sets, syringes, PEG tubes, and NG tubes have specific EnFit ends that can only be used with tube feeding sets. This new safety design will avoid inadvertent administration of enteral feeding into intravenous tubing that can cause life-threatening adverse effects.

Enteral Feeding Pump and Tubing
Enteral feeding is administered to infants and children via a syringe, gravity feeding set, or feeding pump. The method selected is dependent on the nature of the feeding and clinical status of the child.[20]
The most serious complication of enteral feeding is inadvertent respiratory aspiration of gastric contents, causing life-threatening aspiration pneumonia. Other complications include tube clogging, tubing misconnections, and patient intolerance of enteral feeding.[21]
In addition to verifying tube placement as discussed in an earlier section, nurses perform additional interventions to prevent aspiration. The American Association of Critical‐Care Nurses recommends the following guidelines to reduce the risk for aspiration:
Measurement of gastric residual volume (GRV) is performed by using a 60-mL syringe to aspirate stomach contents through the tube. It has traditionally been used to assess aspiration risk with associated interventions such as slowing or stopping the enteral feeding. GRVs in the range of 200–500 mL cause interventions such as slowing or stopping the feeding to reduce risk of aspiration. However, according to recent research, it is not appropriate to stop enteral nutrition for GRVs less than 500 mL in the absence of other signs of intolerance because of the impact on the patient’s overall nutritional status. Additionally, the aspiration of gastric residual volumes can contribute to tube clogging.[23] Follow agency policy regarding measuring gastric residual volume and implementing interventions to prevent aspiration.
Feeding tubes are prone to clogging for a variety of reasons. The risk of clogging may result from tube properties (such as narrow tube diameter), the tube tip location (stomach vs. small intestine), insufficient water flushes, aspiration for gastric residual volume (GRV), contaminated formula, and incorrect medication preparation and administration. A clogged feeding tube can result in decreased nutrient delivery or delayed administration of medication, and, if not corrected, the patient may require additional surgical intervention to replace the tube.[24]
Research supports using water as the best choice for initial declogging efforts. Instill warm water into the tube using a 60‐mL syringe, and apply a gentle back‐and‐forth motion with the plunger of the syringe. Research shows that the use of cranberry juice and carbonated beverages to flush the tube can worsen tube occlusions because the acidic pH of these fluids can cause proteins in the enteral formula to precipitate within the tube. If water does not work, a pancreatic enzyme solution, an enzymatic declogging kit, or mechanical devices for clearing feeding tubes are the best second‐line options.[25]
To prevent enteral tubes from clogging, it is important to follow these guidelines:
In April 2006, The Joint Commission issued a Sentinel Event Alert on tubing misconnections due to enteral feedings being inadvertently infused into intravenous lines with life-threatening results. A color-coded enteral tubing connection design was developed to visually communicate the difference between enteral tubing and intravenous tubing. In addition to tubing design, follow these guidelines to prevent tubing misconnection errors:
Patients should be monitored daily for signs of tube feeding intolerance, such as abdominal bloating, nausea, vomiting, diarrhea, cramping, and constipation. If cramping occurs during bolus feedings, it can be helpful to administer the enteral nutritional formula at room temperature to prevent symptoms.[28] Notify the provider of signs of intolerance with anticipated changes in the prescription regarding the type of formula or the rate of administration. Electrolytes and blood glucose levels should also be monitored, as ordered, for signs of imbalances.[29],[30]
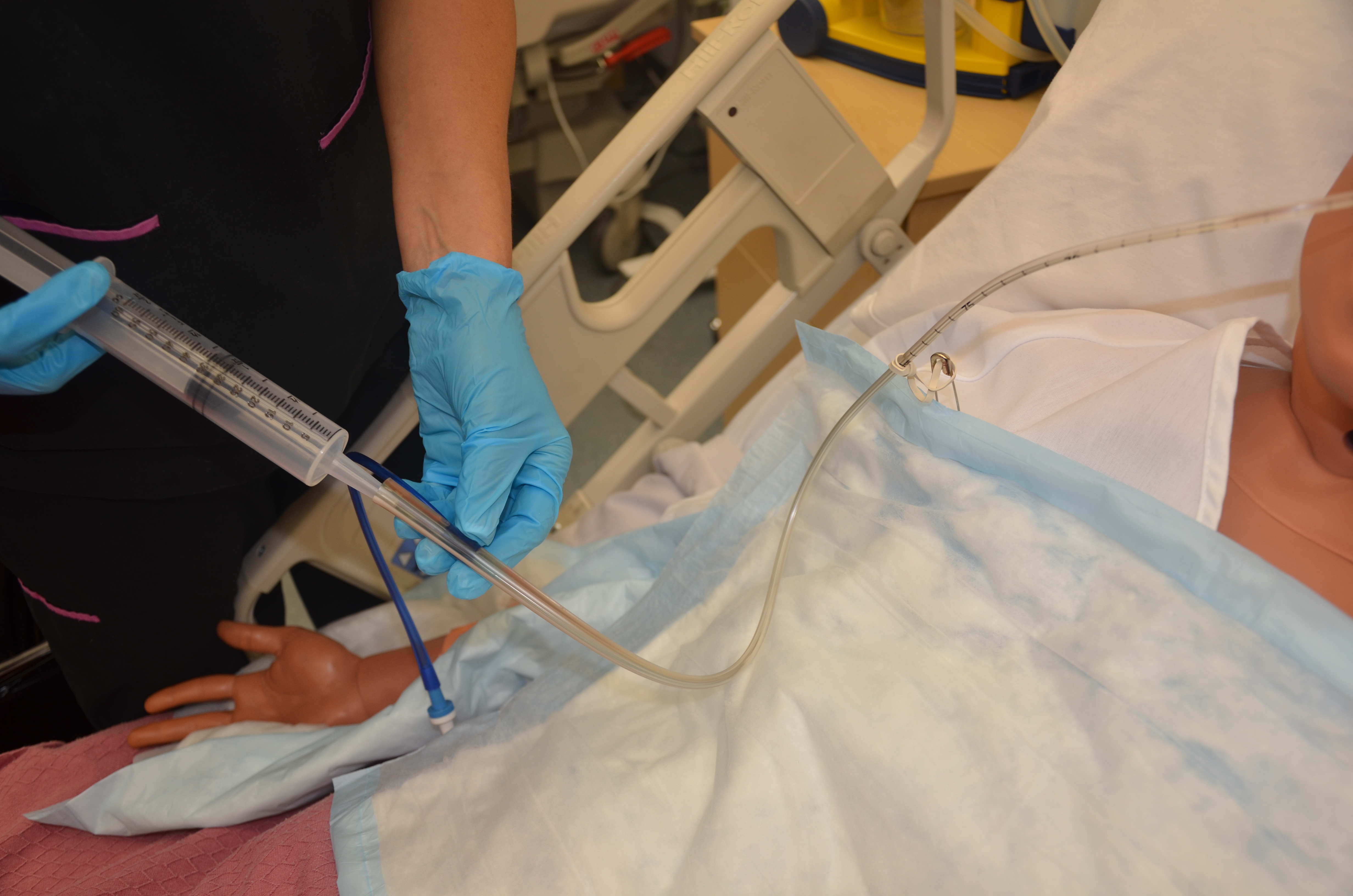
Enteral tubes are routinely flushed to maintain patency. Follow agency policy when flushing a tube. Typically, tap water and a 60-mL syringe are used to flush enteral tubes.[31] See Figure 17.8[32] for an image of a nurse irrigating an NG tube.

Irrigating an NG Tube
The steps for irrigating enteral tubes are typically the following:
NG tubes may be used to remove gastric content, referred to as gastric decompression. In these situations, the stomach is drained by gravity or by connection to a suction pump to prevent nausea, vomiting, gastric distension, or to wash the stomach of toxins. This procedure is commonly used for post-operative patients who have not yet regained peristalsis or for patients with a small bowel obstruction to remove the accumulation of stomach bile. It is also used in the emergency department for patients with some types of poisonings or overdoses and is commonly referred to as “pumping out the stomach.”
For patients receiving suctioning via enteral tubes, the drainage amount and color should be documented every shift.
When caring for patients with enteral tubes, it is important for the nurse to routinely assess and document the patient’s condition.
When a patient is receiving enteral feeding, the nurse should assess the patient’s tolerance of tube feeding.
Focused Interview Questions for Tube Feeding
| Interview Questions | Follow-up |
|---|---|
| How long have you been receiving tube feeding? | Tell me more about why you are receiving tube feeding and how you feel about the tube feeding. (Patients may experience psychosocial reactions to receiving tube feeding that can be addressed with therapeutic communication.) |
| Are you experiencing symptoms of stomach cramping, nausea, vomiting, excess gas, diarrhea, or constipation? | Please describe. |
| Are you experiencing any discomfort where the tube is inserted? | Please describe. |
| Have you noticed any coughing or respiratory symptoms after receiving tube feeding? | Please describe. |
Objective assessments for patients with enteral tubes include assessing skin integrity, tube placement, gastrointestinal function, and for signs of complications:
Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Head of the bed elevated to 45 degrees. Placement of tube verified with measurement of the tube at the nares at 55 cm and gastric aspirate had a pH of 4. Patient tolerated 240 mL of tube feeding by gravity followed by a 30-mL water flush.
Irrigated NG tube with 30 mL of water with no resistance. Patient tolerated flush without symptoms.
NG tube connected to low-intermittent suction (LIS) at 60 mmHg. Output from the NGT is green with a volume of 100 mLs in eight hours.
Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Head of the bed elevated to 45 degrees. Placement of tube verified with measurements of tube at nares at 55 cm and gastric aspirate with a pH of 4. After 100 mLs of tube feeding was infused, the patient complained of feeling full and nauseated. Tube feeding infusion stopped and the head of the bed maintained at a 45-degree angle. Will reassess gastric volume residual in one hour and determine if tube feeding will be resumed.
Attempted to irrigate NG tube with 30 mLs of water, but resistance was felt with procedure. Unable to inject water flush into the NGT. Dr. Smith notified of findings at 1320.
Patient’s abdomen is slightly distended and bowel sounds are hypoactive in all four quadrants. Patient reports increased nausea over the last two hours. NGT connected to low-intermittent suction (LIS) at 60 mmHg. Output from the NGT is mahogany colored with a volume of 800 mLs in eight hours. Dr. Smith notified of findings at 1640.
Use the checklist below to review the steps for completion of the “NG Tube Enteral Feeding by Gravity with Irrigation.”

Disclaimer: Always review and follow agency policy regarding this specific skill.
Verify the provider’s order.
Gather supplies: stethoscope, gloves, towel, irrigating solution (usually water), and irrigation set with irrigating syringe, pH tape, and prescribed tube feeding.
Perform safety steps:
Don the appropriate PPE as indicated.
Perform abdominal and nasogastric tube assessment:
Check for tube placement:
Draw up 30 mL of water in a 60-mL syringe. (If applicable, use sterile water according to agency policy.)
Connect the syringe to the tubing port (not the blue pigtail).
Instill 30 mL water.
Reconnect the plug tube or clamp tube.
Remove the plunger from the syringe and attach the syringe to the NG tube.
Complete tube feeding administration:
Disconnect the syringe and plug the NG tube.
Maintain the patient at or above a 30-degree angle for a minimum of one hour to prevent aspiration. Ask the patient if they have any questions and thank them for their time.
Perform hand hygiene.
Ensure safety measures when leaving the room:
Document assessment findings and report any concerns according to agency policy. When documenting the procedure, include the following:
Use the checklist below to review the steps for completion of the “NG Suction.”
Disclaimer: Always review and follow agency policy regarding this specific skill.
Verify the provider’s order.
Gather supplies: nonsterile gloves.
Perform safety steps:
Don the appropriate PPE as indicated.
Perform abdominal and nasogastric tube assessment:
Rationale: Performing a nasogastric and abdominal assessment is important for determining signs of complications such as skin breakdown and necessity for suction.
Don gloves.
Attach the NG tube to the suction canister.
Set the rate of suction according to provider order:
Monitor canister output and document color, odor, consistency, and amount.
Perform hand hygiene.
Ensure safety measures when leaving the room:
Document the procedure and related assessment findings. Report any concerns according to agency policy.
(Answers to “Learning Activities” can be found in the “Answer Key” at the end of the book. Answers to interactive activity elements will be provided within the element as immediate feedback.)
As you are administering tube feeding to your patient, they complain of feeling full. What is the next step to take?
Continue with administering the tube feeding.
Stop the tube feeding and check the gastric residual.
Stop the tube feeding and waste the remaining feeding.
Slow or stop the infusion based on the patient’s response.




Nutrition provided directly into the gastrointestinal (GI) tract through an enteral tube that bypasses the oral cavity.
Stomach contents aspirated with a 60-mL syringe, typically performed for patients receiving enteral feeding to assess aspiration risk with associated interventions such as slowing or stopping tube feeding. GRVs in the range of 200–500 mL should raise concern and lead to the implementation of measures to reduce risk of aspiration.
Using suctioning through a nasogastric tube to remove the contents of the stomach.
Licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Your browsing activity is empty.
Activity recording is turned off.
See more...