
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_aboard_USNS_Comfort_(T-AH_20).jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_in_a_two-week-old_female.jpg){kind=link}
Copyright Notice
Licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Bookshelf ID: NBK593206

An official website of the United States government

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Open Resources for Nursing (Open RN); Ernstmeyer K, Christman E, editors. Nursing Skills [Internet]. Eau Claire (WI): Chippewa Valley Technical College; 2021.
The neurological system is a complex and intricate system that affects all body functions. A neurological assessment includes collecting subjective and objective data through an interview and detailed physical examination of the central nervous system and the peripheral nervous system. Let’s begin by reviewing the anatomy of the neurological system.
When completing a neurological assessment, it is important to understand the functions performed by different parts of the nervous system while analyzing findings. For example, damage to specific areas of the brain, such as that caused by a head injury or cerebrovascular accidents (i.e., strokes), can cause specific deficits in speech, facial movements, or use of the extremities. Damage to the spinal cord, such as that caused by a motor vehicle accident or diving accident, will cause specific motor and sensory deficits according to the level where the spinal cord was damaged.
The nervous system is divided into two parts, the central nervous system and the peripheral nervous system. See Figure 6.1[1]for an image of the entire nervous system. The central nervous system (CNS) includes the brain and the spinal cord. The brain can be described as the interpretation center, and the spinal cord can be described as the transmission pathway. The peripheral nervous system (PNS) consists of the neurological system outside of the brain and spinal cord, including the cranial nerves that branch out from the brain and the spinal nerves that branch out from the spinal cord. The peripheral nervous system can be described as the communication network between the brain and the body parts. Both parts of the nervous system must work correctly for healthy body functioning.

Central and Peripheral Nervous Systems
There major regions of the brain are the cerebrum and cerebral cortex, the diencephalon, the brain stem, and the cerebellum. See Figure 6.2[2] for an illustration of the cerebellum and the lobes of the cerebrum.

Regions of the Brain
The largest portion of our brain is the cerebrum. The cerebrum is covered by a wrinkled outer layer of gray matter called the cerebral cortex. See Figure 6.3[3] for an image of the cerebral cortex. The cerebral cortex is responsible for the higher functions of the nervous system such as memory, emotion, and consciousness. The corpus callosum is the major pathway of communication between the right and left hemispheres of the cerebral cortex. The cerebral cortex is further divided into four lobes named the frontal, parietal, occipital, and temporal lobes.[4] Each lobe has specific functions.

Cerebral Cortex
The frontal lobe is associated with movement because it contains neurons that instruct cells in the spinal cord to move skeletal muscles. The anterior portion of the frontal lobe is called the prefrontal lobe, and it provides cognitive functions such as planning and problem-solving that are the basis of our personality, short-term memory, and consciousness. Broca’s area is also located in the frontal lobe and is responsible for the production of language and controlling movements responsible for speech.[5]
The parietal lobe processes general sensations from the body. All of the tactile senses are processed in this area, including touch, pressure, tickle, pain, itch, and vibration, as well as general senses of the body, such as proprioception (the sense of body position) and kinesthesia (the sense of movement).[6]
The temporal lobe processes auditory information and is involved with language comprehension and production. Wernicke’s area and Broca’s area are located in the temporal lobe. Wernicke’s area is involved in the comprehension of written and spoken language, and Broca’s area is involved in the production of language. Because regions of the temporal lobe are part of the limbic system, memory is also an important function associated with the temporal lobe.[7] The limbic system is involved with our behavioral and emotional responses needed for survival, such as feeding, reproduction, and the fight – or – flight responses.
The occipital lobe primarily processes visual information.[8]
Information from the rest of the central and peripheral nervous system is sent to the cerebrum through the diencephalon, with the exception of the olfactory nerve that connects directly to the cerebrum.[9] See Figure 6.4[10] for an illustration of the diencephalon deep within the cerebrum. The diencephalon contains the hypothalamus and the thalamus.

The Diencephalon Containing the Hypothalamus and the Thalamus.
The hypothalamus helps regulate homeostasis such as body temperature, thirst, hunger, and sleep. The hypothalamus is also the executive region in charge of the autonomic nervous system and the endocrine system through its regulation of the anterior pituitary gland. Other parts of the hypothalamus are involved in memory and emotion as part of the limbic system.[11]
The thalamus relays sensory information and motor information in collaboration with the cerebellum. The thalamus does not just pass the information on, but it also processes and prioritizes that information. For example, the portion of the thalamus that receives visual information will influence what visual stimuli are considered important enough to receive further attention from the brain.[12]
The brain stem is composed of the pons and the medulla. The pons and the medulla regulate several crucial autonomic functions in the body, including involuntary functions in the cardiovascular and respiratory systems, vasodilation, and reflexes like vomiting, coughing, sneezing, and swallowing. Cranial nerves also connect to the brain through the brain stem and provide sensory input and motor output.[13]
The cerebellum is located in the posterior part of the brain behind the brain stem and is responsible for fine motor movements and coordination. For example, when the motor neurons in the frontal lobe of the cerebral cortex send a command down the spinal cord to initiate walking, a copy of that instruction is also sent to the cerebellum. Sensory feedback from the muscles and joints, proprioceptive information about the movements of walking, and sensations of balance are sent back to the cerebellum. If the person becomes unbalanced while walking because the ground is uneven, the cerebellum sends out a corrective command to compensate for the difference between the original cerebral cortex command and the sensory feedback.[14]
The spinal cord is a continuation of the brain stem that transmits sensory and motor impulses. The length of the spinal cord is divided into regions that correspond to the level at which spinal nerves pass through the vertebrae. Immediately adjacent to the brain stem is the cervical region, followed by the thoracic, the lumbar, and finally the sacral region.[15] The spinal nerves in each of these regions innervate specific parts of the body. See more information under the “Spinal Nerves” section.
Review the anatomy of the brain using following supplementary video.

The peripheral nervous system (PNS) consists of cranial nerves and spinal nerves that exist outside of the brain, spinal cord, and autonomic nervous system. The main function of the PNS is to connect the limbs and organs to the central nervous system (CNS). Sensory information from the body enters the CNS through cranial and spinal nerves. Cranial nerves are connected directly to the brain, whereas spinal nerves are connected to the brain via the spinal cord.
Peripheral nerves are classified as sensory nerves, motor nerves, or a combination of both. Sensory nerves carry impulses from the body to the brain for processing. Motor nerves transmit motor signals from the brain to the muscles to cause movement.
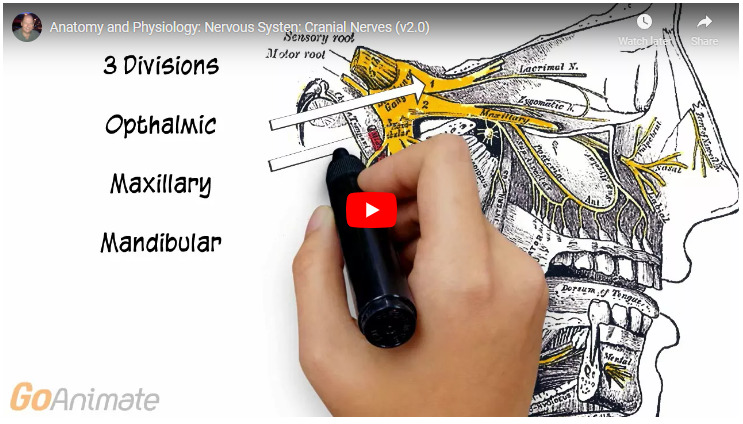
Cranial nerves are directly connected from the periphery to the brain. They are primarily responsible for the sensory and motor functions of the head and neck. There are twelve cranial nerves that are designated by Roman numerals I through XII. See Figure 6.5[17] for an image of cranial nerves. Three cranial nerves are strictly sensory nerves; five are strictly motor nerves; and the remaining four are mixed nerves.[18] A traditional mnemonic for memorizing the names of the cranial nerves is “On Old Olympus Towering Tops A Finn And German Viewed Some Hops,” in which the initial letter of each word corresponds to the initial letter in the name of each nerve. A second popular mneumonic to assist with memorization is “Oh Once One Takes The Anatomy Final Very Good Vacations Are Heavenly”.

Cranial Nerves
There are 31 spinal nerves that are named based on the level of the spinal cord where they emerge. See Figure 6.6[21] for an illustration of spinal nerves. There are eight pairs of cervical nerves designated C1 to C8, twelve thoracic nerves designated T1 to T12, five pairs of lumbar nerves designated L1 to L5, five pairs of sacral nerves designated S1 to S5, and one pair of coccygeal nerves. All spinal nerves are combined sensory and motor nerves. Spinal nerves extend outward from the vertebral column to innervate the periphery while also transmitting sensory information back to the CNS.[22]

Spinal Cord and Spinal Nerves
Each spinal nerve innervates a specific region of the body:

When a patient experiences a spinal cord injury, the degree of paralysis can be predicted by the location of the spinal cord injury. It is also important to remember when a patient has a spinal cord injury and their motor nerves are damaged, their sensory nerves may still be intact. If this occurs, the patient can still feel sensation even if they can’t move the extremity. Therefore, don’t assume that a paralyzed patient cannot feel pain in the affected extremity because this is not always the case.
The nervous system receives information about the environment around us (sensation) and generates responses to that information (motor responses). The process of integration combines sensory perceptions and higher cognitive functions such as memories, learning, and emotion while producing a response.
Sensation is defined as receiving information about the environment. The major senses are taste, smell, touch, sight, and hearing. Additional sensory stimuli are also provided from inside the body, such as the stretch of an organ wall or the concentration of certain ions in the blood.[29]
The nervous system produces a response based on the stimuli perceived by sensory nerves. For example, withdrawing a hand from a hot stove is an example of a response to a painfully hot stimulus. Responses can be classified by those that are voluntary (such as contraction of a skeletal muscle) and those that are involuntary (such as contraction of smooth muscle in the intestine). Voluntary responses are governed by the somatic nervous system, and involuntary responses are governed by the autonomic nervous system.[30]
Integration occurs when stimuli received by sensory nerves are communicated to the nervous system and the information is processed, leading to the generation of a conscious response. Consider this example of sensory integration. A batter in a baseball game does not automatically swing when they see the baseball thrown to them by the pitcher. First, the trajectory of the ball and its speed will need to be considered before creating the motor response of a swing. Then, integration will occur as the batter generates a conscious decision of whether to swing or not. Perhaps the count is three balls and one strike, and the batter decides to let this pitch go by in the hope of getting a walk to first base. Perhaps the batter is afraid to strike out and doesn’t swing, or maybe the batter learned the pitcher’s nonverbal cues the previous time at bat and is confident to take a swing at an anticipated fast ball. All of these considerations are included as part of the batter’s integration response and the higher level functioning that occurs in the cerebral cortex.[31]

The neurological exam is a clinical assessment of the functioning of the central nervous system (CNS) and peripheral nervous system (PNS). See Figure 6.7[1] for an image of the anatomical underpinnings of the neurological exam. Several tests are available when performing a neurological assessment; the tests included in the assessment are selected based on the patient’s medical condition and the neurological symptoms they are experiencing. The range of tests that can be included in a neurological exam include evaluation of mental status, cranial nerves, sensory functioning, motor strength, cerebellar functioning, and reflexes. The mental status exam assesses the higher cognitive functions such as memory, orientation, and language associated with the cerebrum and cerebral cortex. The cranial nerve exam tests the sensory and motor functioning of the 12 cranial nerves that connect to the diencephalon and the brain stem. The sensory response and motor strength tests evaluate functions associated with the spinal nerves. The cerebellar function tests evaluate balance, muscle tone, and coordination of voluntary movements. Deep tendon reflexes may also be used to assess the health of the nervous system.[2] Each of these components of a neurological exam is further described in the remaining sections of this chapter.

Anatomical Underpinnings of Neurological Exam
The type of neurological exam performed is based on the patient’s reason for seeking care, their current medical condition, and the practice setting.
Routine neurological exams performed by registered nurses during their daily clinical practice include assessing mental status and level of consciousness, pupillary response, motor strength, sensation, and gait. The Glasgow Coma Scale is also frequently used to objectively monitor level of consciousness in patients with neurological damage such as a head injury or cerebrovascular accident (i.e., stroke).[3]
A comprehensive neurologic exam is performed on patients with a neurological concern. This exam is more extensive and may be performed in specialty settings or by advanced practice nurses. In addition to the components included in a routine neurological exam, the examiner may also assess cranial nerves, detailed cerebellar function, deep tendon reflexes, and complete a Mini-Mental State Exam (MMSE).
Periodic reevaluations are performed by registered nurses when the patient has experienced an acute injury or illness causing neurological deficits that require frequent monitoring for change in condition. For example, a patient admitted to the hospital for an acute cerebrovascular accident (i.e., stroke) will have their neurological status rechecked and documented frequently according to agency policy. See Figure 6.8[4] of a nurse assessing a patient’s neurological status in an intensive care unit.

Nurse Assessing Patient’s Neurological Status in ICU
Routine assessment of a patient’s mental status by registered nurses includes evaluating their level of consciousness, as well as their overall appearance, general behavior, affect and mood, general speech, and cognitive performance.[1],[2] See the “General Survey Assessment” chapter for more information about an overall mental status assessment.
Level of consciousness refers to a patient’s level of arousal and alertness.[3] Assessing a patient’s orientation to time, place, and person is a quick indicator of cognitive functioning. Level of consciousness is typically evaluated on admission to a facility to establish a patient’s baseline status and then frequently monitored every shift for changes in condition.[4] To assess a patient’s orientation status, ask, “What is your name? Where are you? What day is it?” If the patient is unable to recall a specific date, it may be helpful to ask them the day of the week, the month, or the season to establish a baseline of their awareness level.
A normal level of orientation is typically documented as, “Patient is alert and oriented to person, place, and time,” or by the shortened phrase, “Alert and oriented x 3.” [5] If a patient is confused, an example of documentation is, “Patient is alert and oriented to self, but disoriented to time and place.”
There are many screening tools that can be used to further objectively assess a patient’s mental status and cognitive impairment. Common screening tools used frequently by registered nurses to assess mental status include the Glasgow Coma Scale, the National Institutes of Health Stroke Scale (NIHSS), and the Mini-Mental State Exam (MMSE).
The Glasgow Coma Scale (GCS) is a standardized tool used to objectively assess and continually monitor a patient’s level of consciousness when damage has occurred, such as after a head injury or a cerebrovascular accident (stroke). See Figure 6.9[6] for an image of the Glasgow Coma Scale. Three primary areas assessed in the GCS include eye opening, verbal response, and motor response. Scores are added from these three categories to assign a patient’s level of responsiveness. Scores ranging from 15 or higher are classified as the best response, less than 8 is classified as comatose, and 3 or less is classified as unresponsive.

Glasgow Coma Scale
The National Institutes of Health Stroke Scale (NIHSS) is a standardized tool that is commonly used to assess patients suspected of experiencing an acute cerebrovascular accident (i.e., stroke).[7] The three most predictive findings that occur during an acute stroke are facial drooping, arm drift/weakness, and abnormal speech. Use the following hyperlink to view the stroke scale.
A commonly used mnemonic regarding assessment of individuals suspected of experiencing a stroke is “BEFAST.” BEFAST stands for Balance, Eyes, Face, Arm, and Speech Test.
The Mini-Mental Status Exam (MMSE) is commonly used to assess a patient’s cognitive status when there is a concern of cognitive impairment. The MMSE is sensitive and specific in detecting delirium and dementia in patients at a general hospital and in residents of long-term care facilities.[8] Delirium is acute, reversible confusion that can be caused by several medical conditions such as fever, infection, and lack of oxygenation. Dementia is chronic, irreversible confusion and memory loss that impacts functioning in everyday life.
Prior to administering the MMSE, ensure the patient is wearing their glasses and/or hearing aids, if needed.[9] A patient can score up to 30 points by accurately responding and following directions given by the examiner. A score of 24-30 indicates no cognitive impairment, 18-23 indicates mild cognitive impairment, and a score less than 18 indicates severe cognitive impairment. See Figure 6.10[10] for an image of one of the questions on the MMSE regarding interlocking pentagons.

MMSE Question on Interlocking Pentagons
When performing a comprehensive neurological exam, examiners may assess the functioning of the cranial nerves. When performing these tests, examiners compare responses of opposite sides of the face and neck. Instructions for assessing each cranial nerve are provided below.
Ask the patient to identify a common odor, such as coffee or peppermint, with their eyes closed. See Figure 6.11[1] for an image of a nurse performing an olfactory assessment.

Assessing Cranial Nerve I (Olfactory)
Be sure to provide adequate lighting when performing a vision assessment.
Far vision is tested using the Snellen chart. See Figure 6.12[2] for an image of a Snellen chart. The numerator of the fractions on the chart indicate what the individual can see at 20 feet, and the denominator indicates the distance at which someone with normal vision could see this line. For example, a result of 20/40 indicates this individual can see this line at 20 feet but someone with normal vision could see this line at 40 feet.

Snellen Chart
Test far vision by asking the patient to stand 20 feet away from a Snellen chart. Ask the patient to cover one eye and read the letters from the lowest line they can see.[3] Record the corresponding result in the furthermost right-hand column, such as 20/30. Repeat with the other eye. If the patient is wearing glasses or contact lens during this assessment, document the results as “corrected vision.” Repeat with each eye, having the patient cover the opposite eye. Alternative charts are available for children or adults who can’t read letters in English.
Near vision is assessed by having a patient read from a prepared card from 14 inches away. See Figure 6.13[4] for a card used to assess near vision.

Assessing Near Vision
Cranial nerve III, IV, and VI (oculomotor, trochlear, abducens nerves) are tested together.

Assessing Pupillary Reaction to Light

Assessing Eye Convergence and Accommodation

Read more details about assessing the Pupillary Light Reflex.

Assessing Trigeminal Sensory Function

Assessing Trigeminal Motor Function

Assessing Motor Function of Facial Nerve

Assessing Sensory Function of Facial Nerve

Assessing Auditory Function

Romberg Test
Ask the patient to open their mouth and say “Ah” and note symmetry of the upper palate. The uvula and tongue should be in a midline position and the uvula should rise symmetrically when the patient says “Ah.” (see Figure 6.22[14]).

Assessing Glossopharyngeal Nerve
Use a cotton swab or tongue blade to touch the patient’s posterior pharynx and observe for a gag reflex followed by a swallow. The glossopharyngeal and vagus nerves work together for integration of gag and swallowing. See Figure 6.23[15] for an image of assessing the gag reflex.

Observing the Gag Reflex
Test the right sternocleidomastoid muscle. Face the patient and place your right palm laterally on the patient’s left cheek. Ask the patient to turn their head to the left while resisting the pressure you are exerting in the opposite direction. At the same time, observe and palpate the right sternocleidomastoid with your left hand. Then reverse the procedure to test the left sternocleidomastoid.
Continue to test the sternocleidomastoid by placing your hand on the patient’s forehead and pushing backward as the patient pushes forward. Observe and palpate the sternocleidomastoid muscles.
Test the trapezius muscle. Ask the patient to face away from you and observe the shoulder contour for hollowing, displacement, or winging of the scapula and observe for drooping of the shoulder. Place your hands on the patient’s shoulders and press down as the patient elevates or shrugs the shoulders and then retracts the shoulders.[16] See Figure 6.24[17] for an image of assessing the trapezius muscle.

Assessing Cranial Nerve XI
Ask the patient to protrude the tongue. If there is unilateral weakness present, the tongue will point to the affected side due to unopposed action of the normal muscle. An alternative technique is to ask the patient to press their tongue against their cheek while providing resistance with a finger placed on the outside of the cheek. See Figure 6.25[18] for an image of assessing the hypoglossal nerve.

Assessing the Hypoglossal Nerve
See Table 6.5 for a comparison of expected versus unexpected findings when assessing the cranial nerves.
Expected Versus Unexpected Findings of an Adult Cranial Nerve Assessment
| Cranial Nerve | Expected Finding | Unexpected Finding (Dysfunction) |
|---|---|---|
| I. Olfactory | Patient is able to describe odor. | Patient has inability to identify odors (anosmia). |
| II. Optic | Patient has 20/20 near and far vision. | Patient has decreased visual acuity and visual fields. |
| III. Oculomotor | Pupils are equal, round, and reactive to light and accommodation. | Patient has different sized or reactive pupils bilaterally. |
| IV. Trochlear | Both eyes move in the direction indicated as they follow the examiner’s penlight. | Patient has inability to look up, down, inward, outward, or diagonally. Ptosis refers to drooping of the eyelid and may be a sign of dysfunction. |
| V. Trigeminal | Patient feels touch on forehead, maxillary, and mandibular areas of face and chews without difficulty. | Patient has weakened muscles responsible for chewing; absent corneal reflex; and decreased sensation of forehead, maxillary, or mandibular area. |
| VI. Abducens | Both eyes move in coordination. | Patient has inability to look side to side (lateral); patient reports diplopia (double vision). |
| VII. Facial | Patient smiles, raises eyebrows, puffs out cheeks, and closes eyes without difficulty; patient can distinguish different tastes. | Patient has decreased ability to taste. Patient has facial paralysis or asymmetry of face such as facial droop. |
| VIII. Vestibulocochlear (Acoustic) | Patient hears whispered words or finger snaps in both ears; patient can walk upright and maintain balance. | Patient has decreased hearing in one or both ears and decreased ability to walk upright or maintain balance. |
| IX. Glossopharyngeal | Gag reflex is present. | Gag reflex is not present; patient has dysphagia. |
| X. Vagus | Patient swallows and speaks without difficulty. | Slurred speech or difficulty swallowing is present. |
| XI. Spinal Accessory | Patient shrugs shoulders and turns head side to side against resistance. | Patient has inability to shrug shoulders or turn head against resistance. |
| XII. Hypoglossal | Tongue is midline and can be moved without difficulty. | Tongue is not midline or is weak. |
The sensory function exam tests the somatic senses, meaning those senses that are consciously perceived. Assessing sensory function includes two components, the sensory response that occurs when stimuli are perceived by afferent nerves in the peripheral nervous system and the cortical processing that occurs in the cerebral cortex of the brain.
Testing of peripheral sensation begins with examining the response to light touch according to regions of the skin known as dermatomes. A dermatome is an area of the skin that is supplied by a single spinal nerve that sends information to the brain for processing. See Figure 6.26[1] for an illustration of color-coded dermatomes according to their associated spinal nerves. See more information about spinal nerves in the “Basic Neurological Concepts” section.

Dermatomes
To test the sensory fields, ask the patient to close their eyes, and then gently touch the soft end of a cotton-tipped applicator on random locations of the skin according to the dermatome region. Instruct the patient to report “Now” when feeling the placement of the applicator. If a patient is unable to feel the sensation of a cotton applicator, an advanced technique is to use ice or even the prick of a pin in comatose patients.
It is not necessary to test every part of the skin’s surface during a routine neurological exam; testing a few distal areas with light touch is usually sufficient. In-depth testing is performed when the patient is exhibiting neurological symptoms such as motor deficits, numbness, tingling, and weakness. See Figure 6.27[2] demonstrating assessment of the sensory response.

Assessing Sensory Response
Cortical processing that occurs in the cerebral cortex of the parietal lobe is assessed using stereogenesis. Stereognosis is the ability to perceive the physical form and identity of a familiar object such as a key or paper clip based on tactile stimuli alone.[3] The person typically uses the finger to move the object around and then correctly names the object.
To perform the stereognosis test, ask the patient to close their eyes; then place a familiar object in their hand and ask them to name it. Each hand should be tested with a different object. See Figure 6.28[4] for an image of a patient being tested for stereognosis.

Assessing Stereognosis
Graphesthesia tests assess both cortical sensation and primary sensation. Graphesthesia is the ability to recognize a tracing on the skin while using the sensation of touch. To test graphesthesia, trace a number or letter on the patient’s outstretched palm and ask them to identify it.
A brief musculoskeletal assessment is performed as part of the neurological assessment to determine the neurological stimulation of bilateral strength. Read more details about muscles and musculoskeletal assessment in the “Musculoskeletal Assessment” chapter. Unequal extremity motor strength can indicate underlying neurological disease or injury. Assessing motor strength includes comparing bilateral hand grasps, upper extremity strength, and lower extremity strength. Keep in mind that extremities on the dominant side are usually slightly stronger than the nondominant side.
To perform a hand grasp test, extend two fingers on both hands toward the patient. Ask the patient to squeeze both of your hands and compare for similar bilateral strength. See Figure 6.29[1] for an image of assessing hand grasp strength.

Assessing for Equal Strength in Bilateral Hand Grasps
To test upper extremity strength, ask the patient to extend their forearms with palms facing upwards. Place your hands on their inner forearms and ask them to pull their arms toward them while you provide resistance. An expected finding is the patient strongly bilaterally pulls against resistance with both arms.
An alternative test is to ask the patient to put their hands in the air with their palms facing you. Place your palms against theirs and ask them to push while you provide resistance. See Figure 6.30[2] for an image of assessing upper body strength.

Assessing for Equal Upper Extremity Strength
To assess lower body strength while the patient is in a seated position, place your hands behind their calves. Ask them to pull backwards with their lower legs while you provide resistance in the opposite direction.
Alternative tests are to place your hands on the patient’s lower thighs and ask them to lift their legs upwards while you provide downward resistance, or place your hands on the top of their feet and ask them to pull their toes upwards while you provide resistance. In a similar manner, you can also place your hands underneath their feet and ask them to press downwards “like pressing the gas pedal of a car,” while providing resistance. Compare lower extremity strength on both sides. See Figure 6.31[3] for images of assessing lower extremity strength.

Assessing for Equal Strength in Lower Extremities
The neurological aspect of motor function is based on the activities of the cerebellum. The cerebellum is responsible for equilibrium, coordination, and the smoothness of movement. Specific tests used to evaluate cerebellar function include assessment of gait and balance, pronator drift, the finger-to-nose test, rapid alternating action, and the heel-to-shin test.
When assessing gait and balance, ask the patient to perform the following actions, using an assistive device if needed:
Steps should be equal with a regular pace while arms are swinging and coordinated with walking. Balance should be maintained. A change in gait, weakness, shuffling, jerky movements, loss of balance, or incoordination of arm swing can indicate a neurological dysfunction. See Figure 6.32[1] for an image of assessing gait and balance.

Assessing Gait and Balance
When performing assessment of gait and balance, be aware that the older patient may have a mild degree of muscle weakness or decreased balance associated with aging. When feasible, obtain the patient’s baseline ability and compare current findings to their baseline.
Assessing for pronator drift helps to detect mild upper limb weakness. Ask the patient to close their eyes and extend both arms at 90 degrees at shoulder level with the palms facing upwards. The patient should try to maintain this position for 20 to 30 seconds. Closing the eyes accentuates the effect because the brain is deprived of visual information about the position of the body and must rely on proprioception. Proprioception is the awareness of body position and movement. The expected finding is both arms will maintain this position equally. If the patient is unable to maintain the position, the result is referred to as a positive pronator drift test. Patients with weakness in one arm will not be able to keep the affected arm raised, and ultimately the palm may begin to pronate (palm facing down). In some patients, the arm may remain supinated but will drop lower than the unaffected arm.
The finger-to-nose test assesses equilibrium and coordination. Place the patient in a seated or standing position and ask them to close their eyes. Instruct the patient to extend their arms outward from the sides of the body, and then touch the tip of the nose with the right index finger and return the arm to extended position. Repeat with the left side and continue to repeat touching the nose with alternating movements by both arms.
The expected finding is the patient will smoothly touch the nose with alternating left and right index fingers and return their arms to an extended position repeatedly. An abnormal result occurs when the patient is unable to alternate fingers or demonstrates the inability to touch the nose. For example, the patient may touch the cheek or other part of the face, or movement may be clumsy with stops and restarts. See Figure 6.33[2] for an image of a finger-to-nose test.

Finger-to-Nose Test
To perform a rapid alternating action test, place the patient in a seated position with palms down on thighs. Ask the patient to turn their hands so their palms face upwards and then quickly return them to a downward position and repeat. Instruct the patient to alternate this movement at a fast pace. The expected finding is the rhythm, rate, and movement are smooth and coordinated as pace increases. An abnormal finding is when the patient is unable to alternate movements or can only do so at a slow pace. See Figure 6.34[3] for an example of the rapid alternating action test.

Rapid Alternating Action Test
An alternative test is to have the patient touch the thumb to each finger on their hand in sequence and gradually increase the pace. Repeat this test on the other hand. See Figure 6.35[4] for an alternative finger touch test.

Alternative Finger Touch Test
To perform a heel-to-shin test, place the patient in a supine position. Ask the patient to place the heel of the right foot just below their left kneecap, and then slide the right heel in a straight line down the shin bone to the ankle. Ask them to repeat this procedure on the left leg. The expected action is a smooth and straight movement of both legs. An abnormal finding is if the heel falls off the lower leg or the patient is not able to complete the movement smoothly in a straight motion. See Figure 6.36[5] for an image of the heel-to-shin test.

Heel-to-Shin Test
Assessment of reflexes is not typically performed by registered nurses as part of a routine nursing neurological assessment of adult patients, but it is used in nursing specialty units and in advanced practice. Spinal cord injuries, neuromuscular diseases, or diseases of the lower motor neuron tract can cause weak or absent reflexes. To perform deep reflex tendon testing, place the patient in a seated position. Use a reflex hammer in a quick striking motion by the wrist on various tendons to produce an involuntary response. Before classifying a reflex as absent or weak, the test should be repeated after the patient is encouraged to relax because voluntary tensing of the muscles can prevent an involuntary reflexive action.
Reflexes are graded from 0 to 4+, with “2+” considered normal:
To observe assessment of deep tendon reflexes, view the following video.
The brachioradialis reflex is used to assess the cervical spine nerves C5 and C6. Ask the patient to support their arm on their thigh or on your hand. Identify the insertion of the brachioradialis tendon on the radius and briskly tap it with the reflex hammer. The reflex consists of flexion and supination of the forearm. See Figure 6.37[2] for an image of obtaining the brachioradialis reflex.

Brachioradialis Reflex
The triceps reflex assesses cervical spine nerves C6 and C7. Support the patient’s arm underneath their bicep to maintain a position midway between flexion and extension. Ask the patient to relax their arm and allow it to fully be supported by your hand. Identify the triceps tendon posteriorly just above its insertion on the olecranon. Tap briskly on the tendon with the reflex hammer. Note extension of the forearm. See Figure 6.38[3] for an image of the triceps reflex exam.

Triceps Reflex
The patellar reflex, commonly referred to as the knee jerk test, assesses lumbar spine nerves L2, L3, and L4. Ask the patient to relax the leg and allow it to swing freely at the knee. Tap the patella tendon briskly, looking for extension of the lower leg. See Figure 6.39[4] for an image of assessing a patellar reflex.

Patellar Reflex
The plantar reflex assesses lumbar spine L5 and sacral spine S1. Ask the patient to extend their lower leg, and then stabilize their foot in the air with your hand. Slide the object along the lateral surface of the sole of the foot toward the toes. Many patients are ticklish and withdraw their foot, so it is sufficient to elicit the reflex by using your thumb to stroke lightly from the sole of the foot toward the toes. If there is no response, use a blunt object such as a key or pen. The expected reflex is flexion (i.e., bending) of the great toe. An abnormal response is toe extension (i.e., straightening), also known as the Babinski reflex. In a child younger than 2 years old, the big toe should bend up and backward toward the top of your foot while the other four toes fan out. This response is normal and doesn’t indicate any problems or abnormalities. In a child older than 2 years old or in a mature adult, the Babinski sign should be absent. All five toes should flex, or curl downward, as if they’re trying to grab something. If this test is conducted on a child older than 2 or an adult and the toes respond like those of a child under two years old, this can indicate an underlying neurological issue. See Figures 6.40, 6.41, 6.42, and 6.43[5],[6],[7],[8] for images of assessing the plantar reflex.

The Plantar Reflex

Plantar Reflex and Babinski Sign

The Babinski Sign in an Adult

The Normal Babinski Reflex in a Newborn


Newborn reflexes originate in the central nervous system and are exhibited by infants at birth but disappear as part of child development. Neurological disease or delayed development is indicated if these reflexes are not present at birth, do not spontaneously resolve, or reappear in adulthood. Common newborn reflexes include sucking, rooting, palmar grasp, plantar grasp, Babinski, Moro, and tonic neck reflexes.
The sucking reflex is common to all mammals and is present at birth. It is linked with the rooting reflex and breastfeeding. It causes the child to instinctively suck anything that touches the roof of their mouth and simulates the way a child naturally eats. See Figure 6.44[11] for an image of the newborn sucking reflex.

Newborn Sucking Reflex
The rooting reflex assists in the act of breastfeeding. A newborn infant will turn its head toward anything that strokes its cheek or mouth, searching for the object by moving its head in steadily decreasing arcs until the object is found. See Figure 6.45[12] for an image of a newborn exhibiting the rooting reflex.

Newborn Rooting Reflex
When an object is placed in an infant’s hand and the palm of the child is stroked, the fingers will close reflexively, referred to as the palmar grasp reflex. A similar reflexive action occurs if an object is placed on the plantar surface of an infant’s foot, referred to as the plantar grasp reflex. See Figure 6.46[13] for an image of the palmar grasp reflex.

Newborn Palmer Grasp Reflex
The Moro reflex is present at birth and is often stimulated by a loud noise. The Moro reflex occurs when the legs and head of the infant extend while the arms jerk up and out with the palms up. See Figure 6.47[14] for an image of an infant exhibiting the Moro reflex.

Newborn Moro Reflex
The asymmetrical tonic neck reflex, also known as the “fencing posture,” occurs when the child’s head is turned to the side. The arm on the same side as the head is turned will straighten and the opposite arm will bend. See Figure 6.48[15] for an image of the tonic neck reflex.

Tonic Neck
Although infants cannot support their own weight, when the soles of their feet touch a surface, it appears as if they are attempting to walk by placing one foot in front of the other foot.
Now that we have reviewed tests included in a neurological exam, let’s review components of a routine neurological assessment typically performed by registered nurses. The neurological assessment begins by collecting subjective data followed by a physical examination.
Subjective data collection guides the focus of the physical examination. Collect data from the patient using effective communication and pay particular attention to what the patient is reporting, including current symptoms and any history of neurological illness. Ask follow-up questions related to symptoms such as confusion, headache, vertigo, seizures, recent injury or fall, weakness, numbness, tingling, difficulty swallowing (called dysphagia) or speaking (called dysphasia), or lack of coordination of body movements.[1]
See Table 6.10a for sample interview questions to use during the subjective assessment
Interview Questions Related to Subjective Assessment of Neurological System
| Interview Questions | Follow-up |
|---|---|
|
Are you experiencing any current neurological concerns such as headache, dizziness, weakness, numbness, tingling, tremors, loss of balance, or decreased coordination?
Have you experienced any difficulty swallowing or speaking? Have you experienced any recent falls? | If the patient is seeking care for an acute neurological problem, use the PQRSTU method to further evaluate their chief complaint. The PQRSTU method is described in the “Health History” chapter. Note: If critical findings of an acute neurological event are actively occurring, such as signs of a stroke, obtain emergency assistance according to agency policy. |
| Have you ever experienced a neurological condition such as a stroke, transient ischemic attack, seizures, or head injury? | Describe the condition(s), date(s), and treatment(s). |
| Are you currently taking any medications, herbs, or supplements for a neurological condition? | Please describe. |
At birth, the neurologic system is not fully developed. The brain is still developing, and the newborn’s anterior fontanelle doesn’t close until approximately 18 months of age. The sensory and motor systems gradually develop in the first year of life. The newborn’s sensory system responds to stimuli by crying or moving body parts. Initial motor activity is primitive in the form of newborn reflexes. Additional information about newborn reflexes is provided in the “Assessing Reflexes” section. As the newborn develops, so do the motor and sensory integration. Specific questions to ask parents or caregivers of infants include the following:
Depending on the child’s age and developmental level, they may answer questions independently or the child’s parent/guardian may provide information. Specific questions for children include the following:
The aging adult experiences a general slowing in nerve conduction, resulting in a slowed motor and sensory interaction. Fine coordination, balance, and reflex activity may be impaired. There may also be a gradual decrease in cerebral blood flow and oxygen use that can cause dizziness and loss of balance. Examples of specific subjective questions for the older adult include the following:
Educate older adults to change positions slowly, especially when standing up from a lying or sitting position. Lightheadedness and loss of balance during these activities increase the risk for falls.
The physical examination of the neurological system includes assessment of both the central and peripheral nervous systems. A routine neurological exam usually starts by assessing the patient’s mental status followed by evaluation of sensory function and motor function. Comprehensive neurological exams may further evaluate cranial nerve function and deep tendon reflexes. The nurse must be knowledgeable of what is normal or expected for the patient’s age, development, and condition to analyze the meaning of the data that is being collected.
Nurses begin assessing a patient’s overall neurological status by observing their general appearance, posture, ability to walk, and personal hygiene in the first few minutes of nurse-patient interaction. For additional information about obtaining an overall impression of a patient’s status while performing an assessment, see the “General Survey” chapter.
Level of orientation is assessed and other standardized tools to evaluate a patient’s mental status may be used, such as the Glasgow Coma Scale (GCS), NIH Stroke Scale, or Mini-Mental State Exam (MMSE). Read more information about these tools under the “Assessing Mental Status” section earlier in this chapter.
The nurse also assesses a patient’s cerebellar function by observing their gait and balance. See the “Assessing Cerebellar Function” section earlier in chapter for more information.
Auscultation refers to the action of listening to sounds from the heart, lungs, or other organs with a stethoscope as a part of physical examination. Auscultation is not typically performed by registered nurses during a routine neurological assessment. However, advanced practice nurses and other health care providers may auscultate the carotid arteries for the presence of a swishing sound called a bruit. Bruits suggest interference with cerebral blood flow that can cause neurological deficits.
Palpation during a physical examination typically refers to the use of touch to evaluate organs for size, location, or tenderness, but palpation during the neurologic physical exam involves using touch to assess sensory function and motor function. Refer to sections on “Assessing Sensory Function,” “Assessing Motor Function,” “Assessing Cranial Nerves,” and “Assessing Reflexes” earlier in this chapter for additional information on how to perform these tests.
See Table 6.10b for a summary of expected and unexpected findings when performing an adult neurological assessment.
Expected Versus Unexpected Findings on Adult Neurological Assessment
| Assessment | Expected Findings | Unexpected Findings (Document and notify provider if new finding*) |
|---|---|---|
| Inspection | Alert and oriented to person, place, and time Symmetrical facial expressions Clear and appropriate speech Ability to follow instructions PERRLA (Pupils are equal, round, and reactive to light and accommodation) Cranial nerves all intact Negative Romberg test Sensory function present Cortical functioning (indicated by stereognosis) intact Good balance Coordinated gait with equal arm swing Finger-to-nose, rapid alternating arm movements, and heel-to-shin performance intact Negative pronator drift test Motor strength in upper and lower extremities equal bilaterally Deep tendon reflexes intact | Not alert and oriented to person, place, and/or time Asymmetrical facial expressions Garbled speech Inability to follow directions Pupils unequal in size or reactivity Deficits in one or more cranial nerve assessments Positive Romberg test Sensory function impaired in one or more areas Stereognosis not intact Poor balance Shuffled or asymmetrical gait with unequal arm swing Unable to complete finger-to-nose, alternating arm movement, or heel-to-shin tests Positive pronator drift test Unequal strength of upper and/or lower extremities One or more deep tendon reflexes are not reactive |
| Critical findings to report immediately and/or obtain emergency assistance: | Change in mental status, pupil responsiveness, facial drooping, slurred words or inability to speak, or sudden unilateral loss of motor strength |
Patient denies any new onset of symptoms of headaches, dizziness, visual disturbances, numbness, tingling, or weakness. Patient is alert and oriented to person, place, and time. Dress is appropriate, well-groomed, and proper hygiene. Patient is cooperative and appropriately follows instructions during the exam. Speech is clear and facial expressions are symmetrical. Glasgow scores at 15. Gait is coordinated and erect with good balance. PERRLA, pupil size 4mm. Sensation intact in all extremities to light touch. Cranial nerves intact x 12. No deficits demonstrated on Mini-Mental Status Exam. Upper and lower extremity strength and hand grasps are 5/5 (equal with full resistance bilaterally). Follows commands appropriately. Cerebellar function intact as demonstrated through alternating hand movements and finger-to-nose test. Negative Romberg and Pronator drift. Balance is stable during heel-to-toe test. Tolerated exam without difficulty.
Patient is alert and oriented to person, place, and time. Speech is clear; affect and facial expressions are appropriate to situation. Patient cooperative with exam and exhibits pleasant and calm behavior. Dress is appropriate, well-groomed, and proper hygiene. Posture remains erect in wheelchair, with intermittent drift to left side. History of CVA with left sided hemiplegia. Bilateral hearing aids in place with corrective lenses on. Pupils are 4mm equal and round. Reaction intact right and accommodation intact right eye. Left pupil 2mm, round nonreactive to light and accommodation. Upper extremity hand grips, nonsymmetrical due to left-sided weakness. Right hand grip and upper extremity strength strong at 4/5. Left lower extremity residual weakness, rated at 1/5, right lower extremity strength 4/5. Sensation intact to light touch bilaterally, R>L. Unable to assess Romberg and Pronator drift.
Begin assessing a patient’s general appearance, posture, ability to walk, personal hygiene, and other general survey assessments during the first few minutes of the initial nurse-patient interaction. When asking the patient to perform specific neurological tests, it is helpful to demonstrate movements for the patient. Explain the purpose and use of any equipment used.
Use the checklist below to review the steps for completion of a routine “Neurological Assessment.”
Disclaimer: Always review and follow agency policy regarding this specific skill.
Gather supplies: penlight. For a comprehensive neurological exam, additional supplies may be needed: Snellen chart; tongue depressor; cotton wisp or applicator; and percussion hammer; objects to touch, such as coins or paper clips; substances to smell, such as vanilla, mint, or coffee; and substances to taste such as sugar, salt, or lemon.
Perform safety steps:
Obtain subjective assessment data related to history of neurological disease and any current neurological concerns using effective communication.
Assess the patient’s behavior, language, mood, hygiene, and choice of dress while performing the interview. Note any hearing or visual deficits and ensure glasses and hearing aids are in place, if needed.
Assess level of consciousness and orientation; use Glasgow Coma Scale if appropriate.
(Optional) Complete Mini-Mental State Examination (MMSE), if indicated.
Assess for PERRLA.
Assess motor strength and sensation.
Assess coordination and balance.
(Optional) Perform a cranial nerve assessment and assess deep tendon reflexes as indicated.
Assist the patient to a comfortable position, ask if they have any questions, and thank them for their time.
Ensure five safety measures when leaving the room:
Perform hand hygiene.
Document the assessment findings and report any concerns according to agency policy.
(Answers to “Learning Activities” can be found in the ‘”Answer Key'” at the end of the book. Answers to interactive activity elements will be provided within the element as immediate feedback.)
A male client has an impairment of cranial nerve II. Specific to this impairment, the nurse would plan to do which of the following to ensure client safety?
Use a loud tone when speaking to the client
Test the temperature of the shower water
Check the temperature of the food prior to eating
Remove obstacles when ambulating
The nurse is performing a mental status examination on a client with confusion. This test assesses which of the following?
Cerebral function
Cerebellar function
Sensory function
Intellectual function

The ability of the eye to adjust from near vision to far vision. Pupils constrict at near vision and dilate at far vision.
Partial or complete loss of smell. This symptom can be related to underlying cranial nerve dysfunction or other nonpathological causes such as a common cold.
A reflex demonstrated as fanning of 4 toes with great toe bending towards top of foot when object slid along sole of foot. Normal in children under 2. Older than 2 through adulthood, all five toes should curl downward
An area located in the frontal lobe that is responsible for the production of language and controlling movements responsible for speech.
A swishing sound heard upon auscultation.
The part of the nervous system that includes the brain (the interpretation center) and the spinal cord (the transmission pathway).
The part of the brain that coordinates skeletal and smooth muscle movement and maintains equilibrium and balance.
The cerebrum is covered by a wrinkled outer layer of gray matter.
A decreased level of consciousness with a score of less than 8 on the Glasgow Coma Scale.
The action of both eyes moving inward as they focus on a close object using near vision.
An area of the skin that is supplied by a single spinal nerve.
Double vision (i.e., seeing two images of a single object).
Difficulty swallowing.
Difficulty speaking.
The autonomic control center of the brain that controls functions such as blood pressure, heart rate, digestive movement, and pain perception.
A person’s sense of movement.
A patient’s level of arousal and alertness, commonly assessed by asking them to report their name, current location, and time.
Nerves in the peripheral nervous system that transmit motor signals from the brain to the muscles to cause movement.
Involuntary, shaky eye movements.
The partial or complete loss of strength, movement, or control of a muscle or group of muscles within a body part that can be caused by brain or spinal injury.
The part of the nervous system that includes the cranial and spinal nerves.
A person’s sense of their body position.
Drooping of the eyelid.
The function of receiving information about the environment. The major senses are taste, smell, touch, sight, and hearing.
Nerves in the peripheral nervous system that carry impulses from the body to the brain for processing.
The ability to perceive the physical form and identity of an object based on tactile stimuli alone.
Relays sensory information and motor information in collaboration with the cerebellum.
Licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Your browsing activity is empty.
Activity recording is turned off.
See more...