

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-.

ABSTRACT
The clinical syndrome of GH deficiency (GHD) is characterized by non-specific features including variable presence of decreased mood and general well-being, reduced bone remodeling activity, change in body fat distribution with increased central adiposity, hyperlipidemia, and increased predisposition to atherogenesis. The goal of GH replacement therapy in adults with GH deficiency is to correct the wide spectrum of associated clinical alterations. The estimated prevalence of GHD is approximately 2-3:10,000 population. GHD is caused by structural pituitary disease or cranial irradiation, and usually occurs in the context of additional features of hypopituitarism. Pituitary adenomas are the most important cause of adult-onset GHD followed by craniopharyngiomas, which combined account for 57% of cases. Less common causes are irradiation, head injury, vascular, infiltrative, infectious. and autoimmune disease. Diagnosing patients with GHD should first of all consider who should be tested for GHD, which includes patients at relevant risk with an intention to treat, and second which stimulation test to be used including the proper diagnostic cut-off concentration of GH. The diagnosis of GHD in adults is then usually straightforward. Dosage of h-GH replacement is dependent on age, and gender with adolescents and women usually requiring an increased dosage. The dose titration is monitored by IGF-I concentrations and apart from that a number of organ end points, which may act as ‘biomarkers’ of the treatment effects. This chapter provides an update on GHD including diagnostic pitfalls, and treatment effect, safety, and monitoring. For complete coverage of all related areas of Endocrinology, please visit our on-line FREE web-text, WWW.ENDOTEXT.ORG.
INTRODUCTION
The term "midget" as description of a proportionate dwarf was first used in 1816, but it was not until 1912, that Harvey Cushing in “The Pituitary Gland” proposed the existence of a "hormone of growth" promoting skeletal growth in children (1). Growth hormone (GH) or somatrophin was first extracted from cadaveric pituitaries in the late 1950es, and other more metabolic actions of this hormone in humans were described soon after by Maurice Raben (2). The purified hormone was initially only used for the treatment of short stature in hypopituitary children, although Raben already in 1962 described general health improvement after injection of GH in a hypopituitary adult (2). Further, increasing knowledge of GH effects in adults was brought forward by the introduction in 1962 by Utiger et al of a radioimmunoassay for measuring GH in human serum (3).
The clinical syndrome of GH deficiency in adults is a consequence of decreased secretion of GH from the anterior pituitary. Until thirty years ago it was widely held that GH deficiency had little pathophysiological consequence despite the previously mentioned earlier anecdotal reports suggesting presence of GH-remediable symptoms of fatigue and decreased general well-being which responded to GH replacement (2). In retrospect, these observations of more than fifty years ago described quite precisely the later well-known classical features of the GH deficiency syndrome. However, the imitated supplies of cadaveric GH and the focus on pediatric usage resulted in delayed further elucidation of the adult GH deficiency state. The measurement of serum GH and the production of recombinant human GH (rhGH) in 1981 made studies of GH concentrations in adults as well as effects on the human body of GH deficiency possible, and clinical studies on replacement with rhGH could begin.
The initial pivotal trials of GH replacement therapy in adult hypopituitary patients were published in 1989 (4, 5). Numerous subsequent studies have provided compelling evidence for the existence of a syndrome of adult GH deficiency (6-8). This is characterized by the variable presence of decreased exercise tolerance, decreased mood and general well-being, reduced bone remodeling activity, change in body fat distribution with increased central adiposity, hyperlipidemia, and increased predisposition to atherogenesis. However, it is important to recognize that adult-onset GH deficiency is due to structural pituitary or hypothalamic disease or cranial irradiation for other pathologies and, therefore, usually occurs in the context of additional features of hypopituitarism (9, 10). For this reason, the clinical features attributable to GH deficiency may be compounded by, or directly related to, other pituitary deficiencies. Nonetheless, the fact that GH replacement therapy may favorably alter these clinical features provides considerable surrogate evidence for GH deficiency as a causal factor.
Adult GH deficiency is thus a well-recognized clinical entity. It causes abnormalities in substrate metabolism, bone remodeling, body composition, as well as physical, and psychosocial function. Since the mid 80-ies an improvement has been recognized with GH replacement, and this has gradually been incorporated in clinical routine based on the few short-term initial randomized clinical trials, which led to the first international consensus guidelines from Growth Hormone Research Society in 1997 (11) and updated in 2007 (12).

Less well recognized is the fact that the early clinical trials were based on selected groups of patients with very severe hypopituitarism and therefore had a high a priory likelihood of severe GH deficiency, there were few study participants, short-term treatment, and supraphysiological GH doses were calculated based on the experience from childhood GH deficiency. Despite knowledge of the very high influence of age on the secretion of GH (Fig 1) and subsequently on Insulin-like-Growth Factor-I (IGF-I) the initial adult doses in the studies were nevertheless chosen too high (4, 5). Most of the current recommendations and guidelines over the years have thus been based on subsequent retrospective single center experience or data from large surveillance databases run by the pharmaceutical industry as the best surrogates for efficacy and safety of GH therapy of adult GH deficiency (14). The Hypopituitary Control and Complications Study (HypoCCS) compiled data from 5,893 patients on Humatrope® and reported that significant shifts in diagnostic patterns have occurred over 10 years after approval of the adult GH deficiency indication, with a trend to less severe forms of GH deficiency (15). This was further documented in a recent publication from KIMS (Pfizer’s International Metabolic Database) where data compiled over 20 years were retrieved for a total of 6,069 patients with adult-onset GH deficiency and treated with Genotropin® from six countries (Belgium, Germany, Netherlands, Spain, Sweden, and UK). The degree of confirmed GH deficiency became less pronounced and more patients with co-morbidities and diabetes were considered for GH replacement therapy, possibly reflecting increased knowledge and confidence in GH therapy gained with time. Thus, the effects of 1 year of GH replacement were similar over the entry year periods despite changes in the patients’ baseline characteristics (16).
Also, less well recognized is the fact that new possible indications for testing and treatment of GH deficiency have emerged and these very likely have a lower a priori likelihood of the disease than the severely hypopituitary patients initially investigated thus challenging the diagnostic criteria laid down for severe GH deficiency. Clinicians are therefore now dealing with other patient populations as, e.g. traumatic brain injury, where neither testing nor treatment efficacy have been scrutinized sufficiently (17) and where current guidelines therefore may fail to apply correctly.
This chapter is an update of our chapter from 2017 which was in turn based on the previous chapter on the topic written by John Monson, Antonia Brooke and Scott Akker and the update will describe the diagnostic procedures, as well as the clinical consequences and management of adult patient with GH deficiency. The basic physiology of GH and the pathophysiology of GH deficiency in adults have been dealt with in other Endotext chapters (www.endotext.org).
PREVALENCE, INCIDENCE, AND ETIOLOGY OF GH DEFICIENCY IN ADULTS
The true prevalence and incidence rate of adult-onset GH deficiency is difficult to estimate with certainty. A reasonable estimate of the prevalence may be obtained from prevalence data for pituitary macroadenomas, which approximate to 1-2:10,000 population (20-22). Addition of cases of childhood-onset GH deficiency persisting into adult life gives an overall prevalence of 2-3:10,000 population. Incidence rates have been assessed in a Danish nationwide study based on registries (23), including 1,823 patients who were divided in males and females with childhood and adult onset GH deficiency, respectively. The average incidence rates were for childhood onset males, 2.58 (95% confidence interval (CI), 2.30-2.88), childhood onset females, 1.70 (95% CI, 1.48-1.96), adult-onset males, 1.90 (95% CI, 1.77-2.04), and adult-onset females, 1.42 (95% CI, 1.31-1.54) all per 100,000, which are slightly higher than previously reported (24, 25). The incidence rate in the Danish study was significantly higher in males compared to females in the childhood onset GH deficiency group and in the adult-onset GH deficiency group in the age ranges of 45-64 and 65+years, while there was no significant gender difference in the 18-44 years age group. The etiology spectrum of GH deficiency is summarized in figure 2.

Figure 2.
Congenital and acquired causes of growth hormone deficiency
Pituitary adenomas are statistically the most important cause of adult-onset GH deficiency followed by craniopharyngiomas, which combined account for 57% of cases in the study based on data from KIMS, a multinational, pharmacoepidemiological surveillance database for adult hypopituitary patients receiving GH replacement with Genotropin® (Table 1) (26). Over a decade, there was a decrease in patients enrolled in the surveillance databases with diagnoses of pituitary adenoma (50.2 to 38.6%; P<0.001); craniopharyngioma (13.3 to 8.4%; P=0.005) and pituitary hemorrhage (5.8 to 2.8%; P=0.001); increases in idiopathic GH deficiency (13.9 to 19.3%; P<0.001) and undefined/unknown diagnosis (1.3 to 8.6%; P<0.001) in HypoCCS(15).
Table 1.
Etiology in Patients with GH Deficiency (from the KIMS database)
| Etiology category | Category components | n | Patient-years |
|---|---|---|---|
| Pituitary adenoma | Non-functioning adenoma | 5261 | 28 065 |
| Prolactinoma | |||
| Gonadotropinoma | |||
| Thyrotropinoma | |||
| Cushing's disease | Cushing's disease | 859 | 4814 |
| Acromegaly | Acromegaly | 239 | 1396 |
| Pituitary atrophy | Congenital | 2496 | 10 535 |
| Idiopathic | |||
| Empty sella | |||
| Craniopharyngioma | Craniopharyngioma | 1562 | 8392 |
| Benign tumor/lesion | Hamartoma | 462 | 2114 |
| Cyst | |||
| Meningioma | |||
| Schwannoma | |||
| Aggressive tumor (+hematological neoplasm) | Germ cell tumor | 1135 | 5552 |
| Glioma | |||
| Chordoma | |||
| Sarcoma | |||
| Astrocytoma | |||
| Ependymoma | |||
| Medulloblastoma | |||
| Leukemia | |||
| Lymphoma | |||
| Miscellaneous etiology | Traumatic brain injury | 1969 | 8189 |
| Subarachnoid hemorrhage | |||
| Aneurysm | |||
| Sheehan's syndrome | |||
| Hydrocephalus | |||
| Granulomatosis | |||
| Histiocytosis | |||
| Hypophysitis | |||
| Hemochromatosis | |||
| Missing etiology |
From: Gaillard et al (26)
Irradiation includes both pituitary tumors but also other forms of childhood and adult cranial irradiation. Less common causes of adult hypopituitarism are head injury (27), postpartum ischemic necrosis [Sheehan’s syndrome], pituitary apoplexy, infiltrative diseases, and autoimmune lymphocytic hypophysitis. Traumatic brain injury and subarachnoid hemorrhage are increasingly recognized as a cause of hypopituitarism, in particular GH deficiency, which the recently updated guidelines from American Association of Clinical Endocrinologists and American College of Endocrinology indicated to be one of the most common causes of adult GH deficiency seen in clinical practice (18), although data is conflicting (28). Several anti-cancer drugs modulating the immune system and used for antineoplastic purposes may result in hypophysitis with hypofunction including GH deficiency (29, 30), and the list of drugs influencing GH secretion may be increasing, perhaps also including treatment of patient groups with autoimmune diseases.
Most cases of adult GH deficiency arise in adulthood, but a proportion of them are suffering from childhood onset GH deficiency thus also including congenital causes. The proportion in each clinical center will depend on referral practice. In the Danish nationwide study 27% of GH deficiency patients were of childhood origin (23). The congenital cases (figure 2) are due to structural lesions such as Rathke’s pouch cysts, pituitary hypoplasia, and midline defects, or to functionally deficient GH biosynthesis and release such as pituitary-specific transcription factors (PROP1, POU1F1, HESX1, LHX3, LHX4), and LEPR or IGSF1. Thus, childhood-onset GH deficiency due to proven genetic defects in GH synthesis is never reversible and therefore does not require retesting prior to treatment on adult indication. The reversibility of isolated idiopathic GH deficiency of childhood is on the other hand well established with normal GH responses on dynamic testing in various series being described in between 30 and 70% of subjects with confirmed GH deficiencies in childhood at completion of linear growth (31-33). Therefore, childhood-onset isolated GH deficiency should always be challenged by rigorous re-evaluation of causes and retesting at completion of final height.
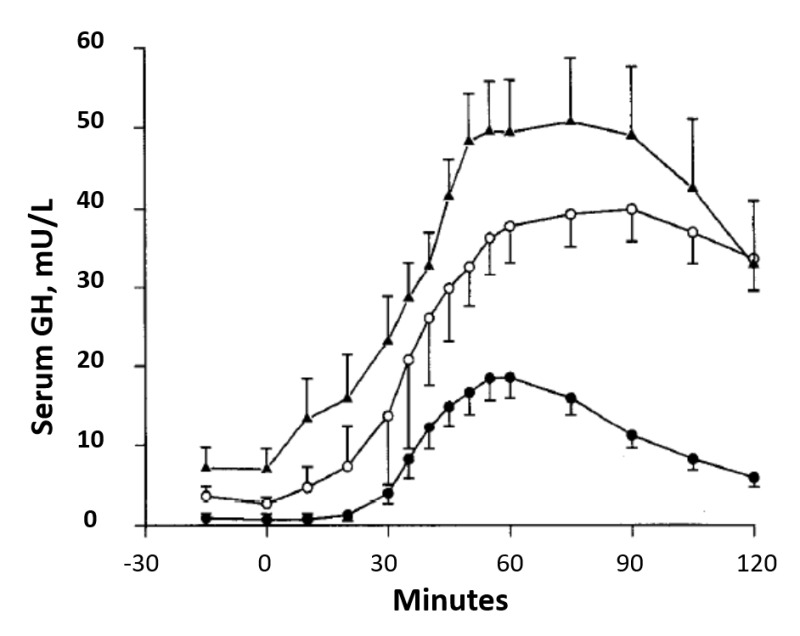
Fig 3.
Mean (±SEM) serum GH response to insulin hypoglycemia in normal subjects (▲) and obese subjects before (●) and after (○) weight loss. From: Rasmussen et al (34).
Isolated idiopathic GH deficiency is not accepted as de novo deficiency in adults at this point in time. This is particularly important in the assessment of non-specific symptoms in ageing or overweight persons without additional evidence of pituitary disease; body mass index of >32 kg/m2 is associated with reduced GH reserve on dynamic testing in approximately 30% of patients but this is reversible with weight loss (Fig 3) (34-37). However, combined deficiency of GH and other anterior pituitary hormones, in the absence of structural disease, may be a feature of an evolving endocrinopathy due to deficiencies of the transcription factors PIT-1 or Prop-1. These cases, and possibly also others, may account for some of the patients with isolated GH deficiency developing into multiple pituitary hormone insufficiencies in 6-65% of cases over time (Fig 4) (38-40).

Fig 4.
Number of patients with GH deficiency and at least one additional pituitary deficit at baseline who developed central hypothyroidism, hypoadrenalism, hypogonadism or ADH deficiency in relation to years from baseline. From: Klose et al (38)
The sequence of loss of pituitary functions is displayed in Fig 5, demonstrating that GH deficiency usually occurs early in the progression of pituitary insufficiency, at least in pituitary adenomas (10). Normalization of GH but also other deficiencies are sometimes observed after selective adenectomy (41-43).

Fig 5.
Sequence of pituitary hormone loss in relation to increasing mass effect from a pituitary tumor. From: Feldt-Rasmussen & Klose (10)
CLINICAL FEATURES OF GH DEFICIENCY IN ADULTS
Adult GH deficiency is associated with an extensive array of non-specific symptoms and physical signs, which are nevertheless recognized by experienced endocrinologists to justify their designation as a clinical syndrome (6-8, 44). Typical symptoms and signs are listed in Table 2.
Table 2.
Typical Symptoms and Signs of the Adult Growth Hormone Deficiency Syndrome
| Body composition increased body fat, particularly central adiposity decreased muscle mass decreased muscle function Cardiovascular and metabolism decreased sweating and poor thermoregulation decreased insulin sensitivity and increased prevalence of impaired glucose tolerance increased total and LDL cholesterol and Apo B. Decreased HDL cholesterol accelerated atherogenesis a variable decrease in cardiac muscle mass impaired cardiac function decreased exercise capacity decreased total and extracellular fluid volume increased concentration of plasma fibrinogen and plasminogen activator inhibitor type I Bones decreased bone mineral density, associated with an increased risk of fracture Quality of Life depressed mood reduced concentration increased anxiety fatigue lack of energy levels low self-esteem increased sick days social isolation lack of positive well being |
Body Composition and Heart
GH deficiency is characterized by substantial changes in body composition with increments in total fat, percentage fat, and particularly visceral fat mass (45-52). Methodologies employed for this purpose have included dual energy X-ray absorptiometry (DEXA) (53), bioelectrical impedance (6-8), CT scan of specific body parts, or the simple measurement of the ratio of waist to hip circumference (52-56) (Table 2) and there is complete concordance among all studies which have examined these aspects in hypopituitary adults. Importantly, although the prevalence of obesity is increased in hypopituitary adults, the increment in visceral fat is also evident in those patients who are non-obese (45). In parallel with changes in fat mass, lean body mass is reduced. The latter may explain the reductions in muscle strength (57-59) and exercise tolerance, which have been documented in adult GH deficiency. The degree to which lean body mass is reduced is difficult to determine because of the reduction in total body water which is also evident in the GH deficiency state; body composition measurements, particularly bioelectrical impedance, may overestimate changes in lean body mass as a consequence of alterations in tissue hydration. Furthermore, the reduction in extracellular water, which is compounded by reduced total body sodium in GH deficiency, may be a major factor underlying the reported reductions in exercise capacity (60-64). To this may be added the effect of reduced left ventricular mass and function which have been described in a number of studies (65-75), although some of these studies on cardiac function in GH deficiency have been less clear.
Glucose Metabolism
In contrast to GH deficiency occurring in children, adult GH deficiency is associated with relative insulin resistance (45, 76-79) and an increased prevalence of impaired glucose tolerance and diabetes mellitus (76). The adverse changes in insulin sensitivity are predictably most obvious in obese patients but are also evident in hypopituitary patients with normal body mass index in whom the inverse relationship between insulin sensitivity and central fat mass, which characterizes the 'metabolic syndrome' is clearly seen (45, 76-79). It is therefore likely that the changes in insulin sensitivity observed in adult GH deficiency are due predominantly to increases in central fat mass. Interestingly, adult subjects with lifetime congenital untreated isolated GH deficiency have reduced β-cell function, no evidence of insulin resistance, and a higher frequency of impaired glucose tolerance (79).Thus, lifetime, untreated isolated GH deficiency increases insulin sensitivity, but impairs β-cell function, and does not provide protection from diabetes (79, 80). It has been postulated that changes in body composition and particularly fat mass might be a consequence of unphysiological glucocorticoid replacement. Against this is the fact that the doses of glucocorticoid replacement used in primary adrenal failure, which are similar to those used in hypopituitarism, are not associated with abnormalities of body composition. However, local tissue exposure to either endogenous or exogenous cortisol may be different in secondary as opposed to primary adrenal failure. The GH/IGF-I axis is now recognized to be an important modulator of the activity of the enzyme 11b hydroxysteroid dehydrogenase Type 1 (11bHSD1) (81). This isoenzyme acts as a predominant reductase, particularly in liver and adipose tissue, increasing the net conversion of inactive cortisone to the active cortisol. The activity of the enzyme is decreased by GH and, as a consequence GH deficiency is associated with a shift in the equilibrium set point in favor of cortisol. It is therefore possible that the increase in central adiposity, which characterizes the GH deficiency state, could be compounded by enhanced exposure to cortisol within adipocytes; hepatic metabolism might be perturbed by a similar mechanism. These mechanisms would tend to increase serum cortisol concentrations in patients receiving hydrocortisone replacement, which is quite often supraphysiological doses, but not in patients with intact ACTH reserve in whom negative feedback would determine maintenance of stable circulating cortisol concentrations. However, GH is also a negative determinant of serum cortisol binding globulin and therefore comparisons of serum total cortisol concentrations between GH deficient and GH replete states are not valid.
Atherosclerosis Risk Factors- Lipids and Hypertension
Adult GH deficiency is associated with an increase in total cholesterol, LDL-cholesterol and apolipoprotein B (4-8, 82, 83). A modest decrement in HDL-cholesterol has also been described in some studies. These changes are evident in both sexes and are quantitatively greater in women. Despite GH deficiency related sodium and water depletion, an increased prevalence of hypertension in adult hypopituitarism has been documented and may be related to a reduced activity of nitric oxide synthase, and consequent increased peripheral vascular resistance, as a result of GH deficiency. The changes in lipoprotein metabolism, body composition, insulin sensitivity, and peripheral vascular resistance indicated above would predict increased atherogenesis in the GH deficiency state. Indeed, several studies have reported an increase in ultrasonographically determined intima-media thickness and plaque formation in large arteries of patients with adult-onset GH deficiency as well as in adults with childhood-onset disease (84, 85).
Bone Mineralization
Decreased bone mineral density is a recognized phenomenon in adult hypopituitary patients (53, 82, 86-92) and is associated with an increased fracture risk (Fig 6) (92-96). Measurements of markers of bone formation and bone resorption are consistent with a low bone turnover state in GH deficiency. Deficits in bone mineral content and density are more striking in adults with childhood-onset GH deficiency and this is likely to be a consequence of failure to achieve genetic potential peak bone mass either because of inadequate GH replacement in childhood or its early cessation at the time of slowing of linear growth (86). Failure to achieve peak bone mass has important implications for the future development of osteoporosis and fracture risk. In the study by Lange et al (96), it was found that patients with idiopathic childhood onset GH deficiency, who at retest in adulthood did not have GH deficiency according to adult criteria, had reduced serum IGF-I and BMD/BMC compared to controls. This observation was also made in the patients who did have persistent GH deficiency in adulthood. The findings may reflect the fact that the present diagnostic criteria for adult GH deficiency (i.e., response to the ITT) do not reflect the clinical consequences of disordered GH-IGF axis in childhood onset GH deficiency young adults who were treated with GH in childhood. Alternatively, despite seemingly adequate GH treatment in childhood an optimal peak bone mass in adolescence may never have been reached in either of the groups. Noteworthy, IGF-I levels correlated with clinical signs of the adult GH deficiency syndrome. The situation in hypopituitarism is further complicated by the frequent accompaniment of gonadal steroid deficiency, often of unknown duration, which has a documented effect on the BMD (97). In addition, glucocorticoid replacement for primary adrenal failure is associated with modest reductions in bone mineral density, but over-replacement in hypopituitary patients does accelerate bone loss (98). Thus, glucocorticoid over-replacement may increase the prevalence of vertebral fractures in patients with untreated GH deficiency. However, treatment of GH deficiency seems to protect the skeleton from the deleterious effects of glucocorticoid overtreatment in hypopituitary patients. Along the same line, data suggest that the characteristics of patients in the various diagnostic groups of hypopituitarism depend on the primary disease which resulted in GH deficiency, and that the clinical expression of GH deficiency does not differ between the groups. Patients with previous hypercortisolism showed more long-term effects of their disease, such as diabetes mellitus, hypertension, and fractures (99), and patients with former Cushing’s disease have more fractures (100). Furthermore, Lange et al reported abnormal bone collagen morphology and decreased bone strength in rats with isolated GH deficiency (101), which might provide a co-explanation for the increased fracture rate in GH deficiency. Whether similar conditions are present in patients with GH deficiency needs further study, but results from a human study of muscle and tendon biopsies from patients with GH deficiency or acromegaly indicated a collagen-stimulating role of local IGF-I in human connective tissue and add to the understanding of musculoskeletal pathology in patients with either high or low GH/IGF-I axis activity (102).
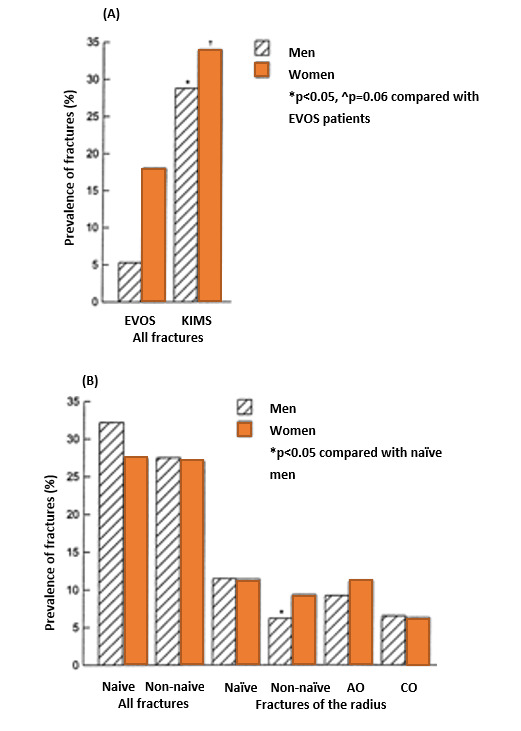
Fig. 6.
Comparisons of the prevalence of (A) all fractures in the EVOS (European Vertebral Osteoporosis Study) participants and in KIMS participants over the age of 60 years and (B) all fractures in naïve and non-naïve KIMS patients and of fractures of the radius in naïve and non-naïve and in patients with adult onset (AO) and childhood onset (CO) disease. From: Wüster et al (92)
Nonetheless, available evidence indicates that qualitatively similar changes in bone mineral density are found in adult-onset isolated GH deficiency as in panhypopituitarism, therefore supporting a role for GH deficiency in the pathogenesis. Furthermore, these abnormalities in bone metabolism and bone density are favorably influenced by GH replacement (see later).
Quality of Life
Decreased psychological well-being and quality of life (QoL) are recognized as particularly important for patients with GH deficiency and from the patients' perspective they have arguably become the major indication for GH replacement therapy. In some countries such as UK, decreased QoL is a needed symptom of a certain quantitative level as measured by validated GH deficiency questionnaires before even considering testing and treatment for GH deficiency according to National Institute for Health and Care Excellence or NICE (103). QoL is also related to a number of other features of GH deficiency. Thus Chikani et al. found subnormal anaerobic capacity, which independently predicted stair-climbing capacity and QoL in adults with GH deficiency. The authors concluded that GH regulates anaerobic capacity, which determines QoL and selective aspects of physical function (Fig 7) (104).

Fig 7.
Relationship between stair-climb performance and anaerobic power (A) and VO2max (B), and between daily step counts quantified by pedometry and anaerobic power (C) and VO2max (D) in the combined groups of 13 adults with GHD (●) and matched normal subjects (○). LBM, lean body mass; VO2max, maximal oxygen consumption. From: Chikani et al (104)
QoL issues have been examined using various generic measures including the Nottingham Health Profile and the Psychological General Well Being Schedule (105-108). These instruments determine various aspects of health-related and needs-based quality of life and the most prevalent findings from various studies have been deficits in the domains of mood, anxiety, and social interaction. In one of the studies the Nottingham Health profile was adapted to a 9-year follow-up study of adults with untreated GH deficiency. During this 9-year study, small but significant declines in health were observed in GH-deficient adults who remained untreated. By contrast, the patients who received GH continuously experienced improvements in energy levels while all other areas of QoL were maintained. The beneficial effects of GH on QoL are therefore maintained with long-term GH replacement and obviate the reduction in QoL seen over time in untreated GH-deficient adults (106). Although these findings are readily apparent in many patients with adult-onset GH deficiency, it has proven more difficult to discern similar phenomena in patients with childhood-onset disease. This may be due to at least two factors. Firstly, standard generic quality of life instruments may be insensitive in the investigation of young people and secondly, there may be a major element of psychological adaptation or decreased expectation when the condition has commenced early in life. In an attempt to improve the reproducibility of studies of QoL in adults with GH deficiency, questionnaires have been developed which focus on those symptoms, which are most frequently documented in hypopituitary adults during extended open interviews.
One such instrument, which is now widely used for the baseline and longitudinal follow-up of patients, is the Quality-of-Life Assessment in Growth Hormone Deficient Adults (QoL-AGHDA) (107-111), which is also the one required by NICE. This is a needs-based instrument consisting of 25 questions with a yes/no answer format and the final score is obtained by summating all the positive responses; a higher score, to a maximum of 25, denotes poorer quality of life. The questionnaire has been shown to be reproducible in a variety of languages and satisfies Rasch analysis criteria for unidimensionality, construct validity, and hierarchical ordering of items (108). In the long-term KIMS study surprisingly, QoL-AGHDA scores increased, indicating worsening of QoL across the entry year periods(16). This possibly reflected a patient selection bias, due to the change in the underlying etiology of GH deficiency: for example, the increase in the proportion of patients with traumatic brain injury or other less defined diagnoses may affect QoL. Alternatively, patients with poor QoL were more likely to receive GH treatment (15).
Mortality
Over the past decades it has been increasingly recognized that hypopituitarism is associated with premature mortality. Studies in Sweden and the UK have demonstrated a two-to-three-fold increase in standardized mortality ratio, most striking in women (112-115). Specific pituitary pathologies, especially craniopharyngioma, may convey an increased mortality rate, which is likely to be independent of specific hormonal deficiencies (114). However, bearing in mind the numerical preponderance of pituitary macroadenomas as the cause of hypopituitarism, the overall findings from these studies favor an increase in morbidity and mortality from macrovascular disease and, in one of the Swedish studies, predominantly cerebrovascular disease (113). The increase in cardiovascular mortality in the initial Swedish study (116) was paralleled by a reduction in deaths from malignant disease in males but this has not been a definite feature of subsequent observations.
Much debate surrounds the mechanism for increased prevalence of vascular disease. These patients were replaced with glucocorticoids, thyroxine, and in some cases gonadal steroids, which prompted the conclusion that untreated GH deficiency was the major causal factor (117). However, this interpretation assumed that replacement of adrenal and thyroid deficiency was optimal and must also take into account that estrogen deficiency may not have been replaced. In fact, replacement, particularly with hydrocortisone, was often supraphysiological (118-120), while thyroxine replacement was more likely underdosed (10, 120-123), and estrogen is often not replaced in females of the fertile age (124). Recent clinical practice has rectified this mistake and consequently hydrocortisone doses are now significantly lower and thyroxine doses significantly higher than when the original mortality data were collected. Anecdotally, a recent paper on lifelong untreated isolated GH deficiency due to a mutation in the GH releasing hormone (GHRH) receptor gene found no alteration of longevity in this highly selected genetic background (125). Nonetheless, the fact that untreated GH deficiency, in the context of varying degrees of hypopituitarism, is associated with an adverse cardiovascular risk profile provides circumstantial evidence for a causative role for GH deficiency to mediate increased rates of vascular disease (45, 54, 77, 84, 85).
DIAGNOSTIC PROCEDURES
GH is secreted in a pulsatile fashion with serum measurements varying between peaks and troughs, the latter falling below the assay detection limit of conventional radioimmunoassays. For this reason, a diagnosis of GH deficiency cannot be made by measurement of baseline serum GH concentration although a single serum GH measurement taken fortuitously at the time of a secretory peak may serve to exclude GH deficiency. Therefore, the diagnosis of GH deficiency is dependent on the demonstration of a subnormal rise in serum GH in response to one or more dynamic stimulation tests. Many diagnostic tests have been developed for GH deficiency, most of them for patients with established hypothalamo-pituitary disease with a high a priori test outcome for deficiency. The same tests are now also used for diagnosing GH deficiency in a number of other potential patient populations raising high risk of misuse and wasting of resources. Further, the technical performance of hormone assays is highly variable among different laboratories(126). Thus, diagnosing patients with GH deficiency should first of all consider who should be tested for GH deficiency, the validity of the chosen stimulation test including the proper diagnostic cut-off concentration of GH, and the availability of local resources and expertise. As stated in the 2019 ACCE/ACE paper, cases with no suggestive history such as hypothalamo-pituitary disease or cranial therapy i.e., cases with a low pretest probability or low a priori likelihood of GH deficiency (18), GH stimulation testing should not be performed.
The recommendations for stimulation testing of patients for adult GH deficiency are provided in the guidelines mentioned in Fig. 8 (11, 12, 18, 19). Noteworthy all guidelines mention the patients eligible for testing as having either hypothalamo-pituitary pathology, verified GH deficiency in childhood, or have had intracranial irradiation. Options include the insulin tolerance test (ITT), glucagon test, and combinations of arginine and GH releasing hormone (GHRH) or GH secretagogues. Recently, the macimorelin test was approved for the diagnosis of adult GH deficiency (127).

Fig 8.
Guideline recommendations for whom to test for GH deficiency.

Fig 9.
Plasma human growth hormone (HGH) and blood glucose concentrations after insulin administered intravenously. (PAR, a hypophysectomized patient; other patients, normal). From: Roth et al (128)
The first description of stimulation of GH upon hypoglycemia was published already in 1963 (128) (Fig 9), and the insulin stimulation test (ITT) is still considered the ‘gold’ standard stimulation test for GH deficiency.
The ITT is the best validated test, and has been demonstrated to distinguish reliably between GH responses in patients with structural pituitary disease and those of age matched controls across the adult age range (Fig 10A) (129). A variety of serum GH cut off points have been used to define GH deficiency. However, an international consensus (convened by the Growth Hormone Research Society) has defined severe GH deficiency in adults as a peak response to ITT of <3 µg/L (11).
It is essential that the ITT is carried out in dedicated units under strict supervision by experienced staff and it is contraindicated in patients with epilepsy and/or ischemic heart disease. The ITT may have a questionable reproducibility, probably due to low degree of robustness to everyday life as it strongly depends on pre-test events as well as on the patient (130, 131). Further, the ITT holds a certain risk especially in inexperienced hands (132), although it is quite safe in experienced centers (133).
A particular advantage of insulin and glucagon testing is the simultaneous assessment of the adequacy of ACTH reserve. Combinations of GHRH and either arginine, pyridostigmine (or GH secretagogues) are the most potent stimuli of GH secretion and normative data for these tests have been set to define GH deficiency (28, 134-136). These tests appear to be reliable and practical, with few contraindications and the GHRH + arginine test may eventually replace ITT as the diagnostic test of choice (134, 137) in European countries. However, peak GH in response to these tests as well as to the glucagon test is highly affected by BMI, and thus BMI related cut off levels are mandatory (135).
Choice of stimulation test may be quite difficult, and the evidence from studies is variable. Furthermore, GHRH is not available in USA, which has prompted reassessment of the use of the glucagon as alternative test when ITT is contraindicated (18, 138-141). However, the diagnostic accuracy of the glucagon stimulation test is unclear especially in patients who are overweight. Recently, the macimorelin test showed promising good overall agreement with the ITT at the same cut point, and seemed unaffected by BMI, age, and sex (127), and is now considered a good alternative.

Fig 10.
Results of tests of GH deficiency in normal (○) and hypopituitary patients (●). From: Hoffman et al (129)
As a result of an age related increase in somatostatinergic tone, spontaneous GH secretion declines by approximately 14% per decade of adult life but this does not alter substantially the response to dynamic tests of GH reserve and the same cut-off GH concentrations can be used across the age range (142). However, several tests pose more risks in elderly individuals (e.g., ITT, glucagon) compared to the young (141, 143), and older people are more likely to be obese with a high waist circumference. They are therefore more at risk of getting a false positive test outcome (144, 145), at least if not lowering the cut-off GH concentration. In general, to avoid misdiagnosing hypopituitary patients with GH deficiency, the importance of using local laboratory assay and test specific cut-off concentrations cannot be overemphasized (28, 146-149).
Severe obesity may decrease the GH response to insulin hypoglycemia to levels suggestive of GH deficiency but this is a completely reversible phenomenon if weight loss is achieved (Fig 3) (34). Body composition is by far the most important factor that needs to be considered when GH responses are evaluated and waist corrected GH-responses may be superior to BMI-corrected cut-offs (130). However, regarding the impact of BMI or waist circumference on GH-responses, further studies are needed to establish cut-off values also considering age, sex and ethnicity. Glucocorticoid therapy, including substitution therapy, probably reduces GH-responses to the GHRH + arginine test in line with the PD–GHRH test (150). Failure to recognize the impact of obesity on stimulated GH secretion may result in a false positive diagnosis of GH deficiency (28, 34, 37, 149, 151) and it is now standard practice that the diagnosis should be made in conjunction with evidence of structural pituitary disease and/or the documentation of additional pituitary hormone deficiencies. The latter provide robust support for a diagnosis of GH deficiency because of the increasing probability of GH deficiency in the presence of one (c.80%) or more (c.90%) additional pituitary trophic hormone deficiencies (152, 153) (Fig 11). Sadly, one publication (154) documented that many centers do not comply with recommendations, since the percent of patients meeting recommended test-specific cut points varied from 32 to 100%, depending on the stimulation test used. There was no mentioning of laboratory or assay specific cut-off concentrations. The study thereby highlights the need for continued education regarding treatment guidelines for adult GH deficiency, including the testing procedures.

Fig 11.
Likelihood of GH deficiency related to number of pituitary hormone deficiencies other than GH deficiency. From: Sönksen PH et al. (155)
GH secretory reserve may also be assessed by measurement of serum concentrations of the GH-dependent peptides IGF-I, IGF binding protein 3 (IGFBP3) and the acid labile subunit of the ternary complex (ALS). Of these, IGF-I is the most sensitive marker of GH action and provides a reliable test of GH reserve in childhood-onset disease. Its diagnostic value for GH deficiency is limited by the fact that between 30 and 40% of individuals with severe GH deficiency of adult-onset will demonstrate a serum IGF-I concentration in the low part of the normal age related reference range (116). Nonetheless, in the absence of liver dysfunction or malnutrition, which may secondarily reduce IGF-I generation, and if determined in the appropriate clinical context of pituitary disease and hypopituitarism, a decreased serum IGF-I provides a strong confirmatory indication for GH deficiency (129).
Testing of patients with suspected non-classical causes of hypopituitarism is much more challenging, since most available evidence of diagnostic reliability has been based on patients with structural hypothalamo-pituitary pathology, genetic causes of GH deficiency, documented GH deficiency in childhood, or brain irradiation. In recent years there has been considerable focus on etiologies previously considered rare causes of hypopituitarism. Published series of hypopituitarism in traumatic brain injury and subarachnoid hemorrhage suggested prevalence rates up to 25-50% (17, 156, 157), and both traumatic brain injury and subarachnoid hemorrhage were subsequently highlighted in the guidelines as new indication for GH testing (12, 19). Still it is notable that the large majority of these patients had isolated deficiencies and in particular isolated GH deficiency (27). Acknowledging the many aforementioned caveats for the diagnosis of GH deficiency these cases may have been strongly overemphasized also because most data were based on only single testing. The fairness of such concerns was evident in a Danish study showing a low concordance of repeated testing for GH deficiency in TBI (Fig 12) (28), which underlines the importance of stringent testing including a second confirmatory test in patients with low a-priory likelihood of GH deficiency. This approach is consistent with the ACCE/ACE 2019 guidelines (18).

Fig 12.
The prevalence of insufficient test responses in the total cohort (A) and in the subgroup undergoing dual testing (B). A, Prevalence of insufficient test responses to either ITT or PD-GHRH/GHRH-arg (i.e., combined tests) in the total cohort of TBI patients (black columns) and healthy controls (white columns), respectively, as defined by either local or guideline-derived cutoffs. Whiskers indicate the 95% CI. GHD was more frequently diagnosed in TBI patients tested by a combined test as compared with ITT, and even more so if guideline cutoff values were applied instead of local cutoffs. The results from healthy controls illustrate the high false-positive rate resulting from application of guideline-derived cutoffs, which was significantly above the generally accepted 2.5% for the combined tests (P = .02). *, P < .005 compared with patients. B, Prevalence of insufficient test responses in the subgroups of patients (black columns, n = 169) and controls (white columns, n = 117) undergoing dual testing, as defined by either local cutoff values or guideline-derived cutoff values. Confirmed insufficiency was defined as a concordant positive result to both the ITT and a combined test. Whiskers indicate the 95% CI. [Reproduced with permission]. From: Klose et al. (28)
Main Conclusions
True GH deficiency is an important clinical entity that should be tested, treated, and managed properly. On the other hand, it is important to avoid false diagnosis, which might lead to unnecessary life-long therapy with GH replacement.
The diagnosis of GH deficiency is rather simple in patients with a typical structural pathology in the hypothalamo-pituitary region, especially in cases of multiple pituitary hormone deficiencies and low IGF-I concentrations, where the likelihood of GH deficiency exceeds 97% (Fig 11), and a stimulation test is rarely indicated (Fig 8). In all other cases a stimulation test is needed for the diagnosis and in some patients 2 tests should be performed in order to avoid the risk of overtreatment on a false basis. The knowledge of one’s own laboratory performance as well as own reference population data with BMI cut offs for control persons is crucial in interpretation of results. The same holds true for the testing of the other hormone axes, some of which have similar challenges in diagnosing correctly in hypothalamo-pituitary disease states.
New indications for GH deficiency testing should not be accepted without prior stringent evaluation of test reliability for the particular condition in question by several tests, and preferably in different laboratories, given that the classical GH deficiency phenotype such as obesity, fatigue and QoL often has other causes than GH deficiency.
Table 3.
Strategy for Diagnosing Adult GH Deficiency for the Purpose of Replacement Therapy
| Assess basis for hypopituitary diagnosis Check if the patient is eligible for GH replacement Measure IGF-I age related reference SDS – if below 0 SDS continue testing Assess number of other pituitary hormone deficiencies Make sure other pituitary hormone deficiencies are properly replaced Choose GH stimulation test(s) Perform stimulation test according to: Guidelines Proper local test validation Own reference cut off based on local assay and normal reference population BMI Other confounders MR/CT scan of pituitary in patients with abnormalities QoL assessment (e.g., QoL-AGHDA)(requirement in UK) Severe GH deficiency as defined by the respective GH stimulation tests (fig. 8) |
GH: Growth Hormone; SDS: Standard Deviation Score; IGF-I: Insulin like Growth factor-I; BMI: Body mass index; MR: Magnetic Resonance; CT: Computer Tomography; QoL: Quality of Life; AGHDA: Adult growth hormone deficiency assessment.
RESPONSE TO GH REPLACEMENT IN ADULT GROWTH HORMONE DEFICIENCY
Quality of Life and Psychological Well-Being
Potentially, the greatest immediate indication for growth hormone supplementation is in patients who are assessed as having impaired QoL, and this is in some countries, such as the UK, a prerequisite for reimbursement (table 4) (103). This recommendation from NICE is unchanged and has not been updated.
Table 4.
NICE Recommendations for Treatment with Growth Hormone
NICE has recommended that recombinant human growth hormone should be used only for adults with severe growth hormone deficiency that is severely affecting their quality of life. To be a part of this group, NICE says a person should:
|
From: NICE guidelines (103)
The early high dose placebo controlled trials suggested that around 50% of these patients demonstrated a significant improvement and a desire to continue with replacement longer term (8). The greatest benefit was shown in patients who had severe GH deficiency and greater distress, in terms of energy and vitality, prior to commencing GH. More recent experience using lower doses with fewer side effects, also indicated clear improvement with wish to continue in >90% of patients selected on the basis of a perceived QoL deficit (53, 158). A six-month course of optimally titrated GH replacement is usually needed before the benefits can be assessed clearly, although many patients show a substantial improvement in QoL within three months. For reasons that are unclear, a small proportion of patients (<20%) may not demonstrate significant subjective benefit in QoL until 9 to 12 months after commencing treatment (159). It is important to recognize that the time taken to achieve a maintenance dose of GH may extend to 12 weeks in some patients and is longer on average in women than in men; this should be recognized in therapeutic trials of GH replacement with a finite time frame. It is clear that the time taken to derive subjective benefit from GH replacement in many patients provides strong evidence against a pure placebo effect in this respect. Furthermore, the duration of benefit in QoL, which has been observed for periods of up to 10 years, is similarly indicative of a therapeutic rather than a placebo phenomenon (106, 111, 160). Patients QoL improves most rapidly in the first 12 months of treatment, but even after this there is continued improvement towards the country specific population mean, with particular improvement in problems socializing, tenseness, and self-confidence, which normalize to the background population (161). The improvement is seen in patients with all etiologies of GH deficiency including previous acromegaly (162-164), isolated GH deficiency (56) and previous Cushing’s disease (99, 100). However, not all aspects of QoL normalize and this is particularly true in patients under 60 yrs of age.
The reasons for the differences in QoL outcome between the early studies and current clinical practice has been the subject of much debate and at least three factors are likely to be particularly relevant. Firstly, the initial randomized control trials utilized GH doses based on body weight or surface area and did not take account of the substantial variation in individual responsiveness to GH occurring as a result of gender and other factors. This strategy resulted in excessive GH doses in men and obese subjects and relative undertreatment of women. The adverse symptoms associated with excess GH doses included arthralgia and myalgia, due to GH-induced anti-natriuresis, and it is probable that these factors may have obscured potential subjective benefit. In addition, it is probable that the strict entry criteria inherent in any placebo-controlled study designed to prove concept may have inadvertently eliminated patients who were most likely to demonstrate a benefit in QoL (Table 3) (164). Finally, the current strategy of GH replacement is not to await the full-blown phenotype to develop, but rather to start replacement as soon as the diagnosis is made, as with any other hormone replacement.
These latter phenomena are readily evident when baseline indices of QoL in patients enrolled into randomized control trials are compared with those of patients commencing GH replacement selectively in the clinical practice setting (53, 158, 165), and even more so with the changed selection of patients eligible for GH replacement over the years (16).
The mechanism for the beneficial effect of GH on well-being and QoL remains speculative (164). GH has been shown to cross the blood brain barrier (166, 167) and to exert physiological effects in the central nervous system as evidenced by the generation of neurotransmitters (166), an effect reduced by progressive aging (168, 169). However, the effects of GH in restoring normal hydration and increasing exercise capacity are additional potential contributors to the positive effects on well-being (170).
Table 5.
Effects of Growth Hormone Replacement Therapy on Quality of Life in Adults in Published Trials
| Reference | GHD onset (etiology) | N | Dosage per day or titration | Duration | Design (Controls) | Tests | Change in QoL in the GHD adults |
|---|---|---|---|---|---|---|---|
| Baum et al (1998) | AO | 40 | 2-6 μg/kg | 18 m | PCDB | NHP PGWB GHQ MMPI-2 Cognition tests | = cognition, QoL |
| Burman et al (1995) | Mostly AO | 36 | 2-4 U | 21 m | PCDB | NHP PGWB HSCL Spousal report | ↑ QoL placebo + GH groups (HSCL) ↑QoL GH group (NHP, spousal report) |
| McGauley et al (1989) | Mostly AO | 24 | 0.07 U/kg | 6 m | PCDB | NHP PGWB GHQ | ↑ subjective well-being ↑ QoL (NHP) ↑ QoL (PGWB) |
| Soares et al (1999) | Not stated | 9 | 0.035 U/kg | 6 m | PCDB | HDS BDI Cognitive tests | ↑ QoL, cognition |
| Attanasio et al (1997) | AO+ CO | 173 | 12.5 μg/kg | 18 m | 6m PCDB 12 m open | NHP | =mobility, energy (6 m) ↑mobility, energy (12m) |
| Beshyah et al (1995) | AO+ CO | 40 | 0.04 U/kg | 18 m | 6m PCDB 12 m open | CPRS GHQ | ↑QoL 12m (CPRS) ↑QoL 6m placebo (GHQ) |
| Caroll et al (1997) | Not stated | 42 | 0.024 (6m) 0.012 (6m) μg/kg | 12 m | 6m PCDB 6m open | NHP PGWB | ↑ QoL on both scales ↑ NHP score in placebo |
| Mahajan et al (2004) | AO+CO | 25 | 0.04 (1m) 0.08 (1m) mg/kg/week, Normal IGF-I | 4 m | PCDB Cross over | NHP HDRS MADRS | =mobility, pain ↑energy and emotional reactions ↓social isolation, sleep disturbance ↓depression |
| Mardh et al (1994) | AO | 124 | Not stated | 12-18 m | 6m PCDB 6-12m open | NHP PGWB | ↑ QoL (NHP) ↑ Well-being |
| Urushihara et al (2007) | AO+CO | 64 | 0.021-0.042-0.083 mg/kg/week, Normal IGF-I | 16 m | 24 weeks DBPC 48 weeks Open | SF-36 | ↑ physical functioning and general health (AO) ↓social functioning and mental health (CO) |
| Wallymahmed et al (1997) | Mostly AO | 32 | 0.018 (1m) 0.035 (5m) U/kg | 12 m | 6m PCDB 6m open | GHD-LFS GHD-IS NHP HADS SES MFS | ↑ Self esteem ↑ Energy and emotional reaction (transient) |
| Bengtsson et al (1993) | AO | 10 | 13-26 μg/kg | 6 m | PCDB Cross-over | CPRS SCL-90 | ↑ QoL (CPRS) = QoL (SCL-90) |
| Degerblad et al (1990) | AO | 6 | 0.07-0.09 U/kg | 3 m | PCDB Cross-over | Mood questionnaires Psychometric Testing | = mood, cognition ↑ vitality, mental alertness |
| Whitehead et al (1992) | AO+ CO | 14 | 0.07 U/kg | 6 m | PCDB Cross-over | PGWB | = QoL, but no ↑ IGF-I |
| Cuneo et al (1998) | Mostly AO | 166 | 0.018 (1 m) 0.036 (11m) U/kg | 12 m | 6m PC 6m open | NHP GHDQ Social history | ↑ QoL 12m (NHP) = QoL (GHDQ) |
| Deijen et al (1998) | CO (men) | 48 | 1-3 U/m2 | 24 m | PC | Psychological Testing | = well-being ↑ memory |
| Florkowski et al (1998) | AO+ CO | 20 | 0.035 U/kg | 3m | Randomized PC Cross-over | DSQ SCL-90 SAS | ↑ QoL placebo + GH groups |
| Giusti et al (1998) | AO | 25 | 0.5-1 U | 6 m | Randomized PC | HDS KSQ | ↑ QoL (HDS) = KSQ |
| Miller et al (2010) | AO (Acromegaly) | 30 | Normal IGF-I | 6 m | Randomized PC | AGHDA SF-36 SQ | ↑ QoL (AGHDA) ↑ vitality, mental health, soc functioning, general health ↓ role limitation |
| Verhelst et al (1997) | Mostly AO | 148 | 0.035 U/kg | 24 m | 6m PC 18m open | NHP Social history | ↑ QoL placebo + GH ↓ sick leave hospitalization |
| Ahmad et al (2001) | AO | 46 | Normal IGF-I | 3 m | Open | AGHDA | ↑ QoL after 1 and 3 m |
| Abs et al (2005) | AO+CO (IGHD) | 1775 | Not stated | 12 m | Open (MPHD) | AGHDA | ↑ QoL IGHD+MPHD IGHD=MPHD |
| Drake et al (1998) | AO | 50 | Normal IGF-I | 6 m | Open | AGHDA | ↑ QoL after 3 and 6 m |
| Follin et al. (2010) | CO (ALL) | 13 | 0.2-0.8 mg/d | 60 m | Open (No GH) | Symptom checklist-90 ISSI | = QoL |
| Gibney et al (1999) | AO+ CO | 11 | 0.025 U/kg | 120 m | Open (No GH) | NHP | ↑ QoL (NHP), energy, emotional reaction |
| Gilchrist et al (2002) | AO+ CO | 61 | Not stated | 108 m | Open (No GH) | NHP PGWB | ↑ energy (NHP) ↑ vitality (PGWB) |
| Hernberg-Stahl et al (2001) | AO | 304 | 0.125-0.25 U/kg | 12 m | Open | AGHDA | ↑ QoL after 1 m, higher after 3 m |
| Höybye et al (2010) | AO (CD) | 1070 | Normal IGF-I | 36 m | Open (NFPA) | AGHDA | ↑ QoL CD+NFPA CD > NFPA |
| Kelestimur et al (2005) | AO (SS) | 143 | Normal IGF-I | 24 m | Open (NFPA) | AGHDA | ↑ QoL SS+NFPA SS=NFPA |
| Klose et al. (2009) | AO (IGHD) | 1152 | Normal IGF-I | 24 m | Open (MPHD) | AGHDA | ↑ QoL IGHD+MPHD IGHD=MPHD |
| Koltowska-H et al (2006) | AO | 1117 | Normal IGF-I | 1 – 8 yrs | Open | AGHDA | ↑ QoL |
| Kreitschmann-Andermahr et al. (2008) | AO+CO (TBI) | 41 | Normal IGF-I | 12 m | Open (NFPA) | AGHDA | ↑ QoL TBI+NFPA GHD TBI = GHD NFPA |
| Link et al. (2006) | CO (ALL) | 14 | Normal IGF-I | 12 m | Open | Neuropsycho- logical testing | = |
| Maiter et al (2006) | AO+CO (irradiated) | 1077 | Normal IGF-I | 12 m 24 m | Open (non-irradiated) | AGHDA | ↑ QoL irradiated+non-irradiated irradiated=non-irradiated |
| Moock et al. (2009) | Mostly AO | 651 | Normal IGF-I | 12 m | Open | AGHDA | ↑ QoL |
| Mukherjee et al (2005) | AO+CO (cancer survivors) | 97 | Normal IGF-I | 3-13 m 24-77 m | Open (pituitary pathology) | PGWB AGHDA | ↑ QoL cancer+pit. GHD cancer survivors = pituitary pathology |
| Mukherjee et al (2005) | AO+CO | 30 | Normal IGF-I | 3 m 6 m | Open | PGWB AGHDA | ↑ QoL |
| Murray et al (1999) | AO + CO | 65 | Normal IGF-I | 8 m | Open | PGWB AGHDA | ↑ QoL |
| Murray et al (2001) | CO (cancer) | 27 | Normal IGF-I | 18 m | Open | PGWB AGHDA | ↑ QoL (large, 3 m) |
| Rosilio et al (2004) | AO + CO | 576 | Normal IGF-I | 12 m 48 m | Open | QLS-H | ↑ QoL |
| Van der Klaauw et al. (2009) | AO (Acromegaly) | 16 | Normal IGF-I | 12 m | Open | HADS MFI-20 NHP AGHDA | = QoL |
| Verhelst et al. (2005) | AO (CP) | 721 | Normal IGF-I | 24 m | Open (NFPA) | AGHDA | ↑ QoL CP+NFPA CP = NFPA |
| Wiren et al (1998) | AO + CO | 71 | 6-12 μg/kg | 20-50 m | Open | NHP PGWB | ↑ QoL |
QoL, quality of life; GHD, growth hormone deficiency; AO, adult onset; CO, childhood onset; ALL, acute lymphoblastic leukemia CP, craniopharyngioma; CS, Cushing’s Disease; NFPA, non-functional pituitary adenoma; SS, Sheehan’s syndrome; TBI, traumatic brain injury; n, number of subjects; PC, placebo-controlled; PCDB, placebo-controlled, double-blind; open, open label; Tests used to quantify QoL ↑, =, ↓, change in QoL parameter in GH-treated patients and when available compared to controls (Modified and updated from Hull and Harvey(171) with permission from the authors). From: Klose et al (164)
Body Composition: Fat Mass, Fat Distribution, and Lean Body Mass
GH replacement produces a significant redistribution of body mass, decreasing body fat, and particularly central fat, and increasing lean body mass (6-9, 172). Body fluid balance is also restored. The beneficial effects of GH on total body fat and its distribution have been examined by means of dual energy X-ray absorptiometry (DEXA), computerized tomography (CT), bioelectrical impedance, and ratio of waist to hip circumference (55, 173) (fig 13) and qualitatively similar results have been obtained with excellent concordance between virtually all reported studies. The restoration of normal total body water may result in an artefactual increment in determinations of lean body mass particularly when the latter is measured by bioelectrical impedance. The abnormal fat distribution in GH deficiency is characterized by an increase in the ratio of waist to hip circumference and during long term follow up, serial measurement of waist circumference provides a simple, rapid and reproducible means of monitoring improvement in body fat distribution.

Fig. 13.
Median waist/hip ratio at 0, 6 and 12 months after commencement of GH replacement, men versus women. From: Data from Drake et al (173)
Reductions in body fat are attributed to the lipolytic effect of GH but additional indirect hormonal effects may be important. The conversion of thyroxine to triiodothyronine was shown to be enhanced by GH in early studies of GH replacement (123, 174) although this is a dose related phenomenon and is less evident with the lower doses in current use. However, levothyroxine replacement has very likely not been optimal (121, 122), and increased dosages have improved the lipids over time (121, 122). Also, the enzyme 11ßHSD1 that reduces cortisone to the active hormone cortisol shows increased activity in the GH deficient state and is normalized by low dose GH replacement (81); the consequent increase in cortisol metabolism may result in reduced tissue specific exposure to glucocorticoid in adipocytes and hepatocytes (81). The latter effect provides an additional explanation for decreased total and central fat mass during GH replacement.
Serum Lipoprotein Profiles
The effect of GH replacement on lipoprotein profiles has been examined in numerous studies using differing dose regimens. Regardless of whether the GH dose has been based on body weight or titrated against serum IGF-I the universal finding has been a reduction of serum total cholesterol, accounted for virtually entirely by a reduction in LDL-cholesterol (48, 69, 160, 175-182). The extent of this reduction is greatest in those patients with higher baseline serum cholesterol (fig 14), and independent on obesity variables (182). The median change in an unselected hypopituitary population is between 0.3 and 0.4 mmol/L (48, 175). Importantly, the improvement in LDL-cholesterol is additive to the effects of HMG CoA reductase inhibitors if the patient is receiving concurrent therapy and possibly even synergistic (173), as well as synergistic with optimization of levothyroxine therapy (120-123). The degree of reduction of serum LDL-cholesterol during GH replacement would predict an overall reduction in cardiovascular events in the range of 20%. In addition, some studies have documented an increase in serum HDL-cholesterol, but serum triglyceride levels remain unchanged. Serum lipoprotein(a) has been shown to increase in some studies in patients who demonstrated favorable changes in LDL-cholesterol (45, 183, 184) but the data remain somewhat contradictory by virtue of lipoprotein(a) assay differences; the overall significance in terms of cardiovascular risk is unclear (185).

Fig 14.
Relationship between the lowering of cholesterol (∆Cholesterol) and the pretreatment serum Cholesterol concentration. Derived from data from Florakis et al (175)
Carbohydrate Metabolism and Insulin Sensitivity
Untreated GH deficiency of adult onset is associated with reduced insulin sensitivity, which is, at least in part, related to increased central adiposity (45, 77). The latter improves within the first 3 months of GH replacement but this does not result in an immediate improvement in insulin sensitivity (45). In fact, because of the antagonistic effects of GH on the actions of insulin mediated by hepatic effects, and the increase in circulating free fatty acids, there is on average a further decline in insulin sensitivity, which subsequently returns to baseline over the first year of GH replacement therapy (77). The decline in insulin sensitivity during GH therapy is associated with a slight elevation of fasting plasma glucose and a parallel increase in glycated hemoglobin, both within the normal reference range. Importantly, the increment in glycated hemoglobin is not evident in patients with prior abnormalities of glucose tolerance but is significantly correlated with baseline body mass index, the latter emphasizing the importance of additional dietary and lifestyle advice in these patients.
Reference to the KIMS database indicates that there is an increased baseline prevalence of impaired glucose tolerance and diabetes mellitus prior to commencing GH replacement but subsequently the incidence of new cases of diabetes is not increased provided the body mass index is accounted for. Thus, a recent study of data from the NordiNet® surveillance database concluded that 4 years' GH-replacement therapy did not adversely affect glucose homeostasis in the majority of adults with GH deficiency (186). Yet, the long-term effects of GH replacement on insulin sensitivity can still not be considered quite clear although they are likely to vary depending on age, duration of pituitary disease, and increase in weight/BMI/waist circumference.
Cardiac Function
The GH/IGF-I axis is a recognized modulator of cardiac function and a positive inotropic effect of GH/IGF-I occurs early in the natural history of acromegaly. In contrast, GH deficiency is associated with a reduction in left ventricular wall mass and cardiac output, which is most evident in childhood-onset disease. The variable discordance between childhood-onset and adult-onset GH deficiency in this regard is likely to be due to additional factors impacting on cardiac morphology in adult-onset, including an increased prevalence of hypertension. GH replacement results in increased left ventricular wall mass, fractional shortening, stroke volume and favorable changes in the echocardiographically determined e/a ratio reflecting improved diastolic function (8, 65-75). In some studies, in adult-onset patients, left ventricular hypertrophy has been documented during GH replacement, confirming further the heterogeneity in response to GH replacement. Importantly, GH replacement does not increase blood pressure; in fact, a modest reduction may be seen in patients with pre-existing hypertension reflecting increased generation of nitric oxide as a result of activation of nitric oxide synthase.
Exercise Capacity and Performance
Increased exercise capacity, as measured by maximal oxygen uptake, power output, and isometric muscle strength, has been observed during GH replacement in GH deficient adults (63, 64, 187, 188). A meta-analysis concluded that evidence from short-term controlled studies failed to support a benefit on muscle strength of GH replacement in GH deficient patients, which is likely to occur over a longer time-course, as seen in open-label studies (188) (Fig 15).
The impact of these changes for individual patients is variable and dependent on age and previous exercise requirements. It is intuitively probable that the improvements depend at least in part on improvements in lean body mass. However, restoration of normal circulating volume may also play a positive role (170). In addition, improvement in psychological well-being might be expected to enhance physical activity whilst the latter may have a reciprocal beneficial effect on well-being.

Fig 15.
Per cent change from baseline in lean body mass (Panel A), fat mass (Panel B), anaerobic power (Panel C) and VO2max (Panel D) following 1 month of placebo and 1 month of GH (randomized controlled study) and 6 months of GH (open-label study) in 18 patients with GH deficiency. From: Chikani et al (170).
Indices of Bone Remodeling and Bone Mineral Density
GH deficiency is associated with reduced activity of bone formation and resorption. GH replacement reverses this situation rapidly resulting in increases in markers of bone formation (e.g., osteocalcin and bone specific alkaline phosphatase) and bone resorption (e.g., urine deoxypyridinoline) (Fig 16) (189).

Fig 16.
Markers of bone turnover during 18 months of GH (▲) treatment in a randomized, placebo- controlled (O), double blinded study. Values are given as means (^S.E.). The P values for differences of change from baseline between GH- and placebo-treated patients are *P, 0:05; **P, 0:01; ***P, 0:001; ****P, 0:0001: Creat, creatinine. From: Sneppen et al (189).
This increase in bone metabolism eventually results in an increase in bone mineral density (BMD) but this is not evident for approximately 18 months of treatment and is preceded by a reduction attributable to an increase in the bone remodeling space (53, 93, 189-197). The fact that BMD increases under the influence of GH replacement at physiological doses provides important surrogate evidence for an etiological role for GH deficiency in mediating the reduced BMD observed in hypopituitarism. The improvement is quantitatively more obvious in men than women despite the achievement of similar serum IGF-I SD scores and therefore constitutes a genuine difference in gender susceptibility (fig 17).

Fig 17.
Bone mineral density of the lumbar spine during long-term GH replacement therapy. From Drake et al (173).
Although the improvement in BMD would predict a reduction in fracture rates confirmation of this necessitates long term follow up. Evidence is now emerging supporting a lower fracture risk with GH replacement (92, 198). A prospective cohort study has shown that GH deficient patients treated with GH before the onset of osteoporosis have a lower fracture risk than those untreated, over a mean follow up of 4.6 years (SD 3.8)(199). Increased fracture risk in child onset GH deficiency women can most likely be explained by interaction between oral estrogen and the GH-IGF-I axis. The adequate substitution rate of testosterone (90%) and GH (94%) may have resulted in significantly lower fracture risk in adult-onset GH deficiency men (198). Finally, although in vitro studies have shown that GH has a direct effect on bone remodeling, present physiological concepts and the results of clinical trials from 1996 to 2008 suggest that the anabolic changes in muscle mass and strength may also contribute to changes in BMD/BMC in GH-treated adult GH deficiency patients (200).
GH REPLACEMENT IN ELDERLY HYPOPITUITARY PATIENTS
Published work indicates that the baseline characteristics and response to GH replacement in hypopituitary patients aged over 65 years are qualitatively similar to those in younger patients (52, 201-203). Importantly, GH deficiency in the elderly is distinguishable on dynamic tests from the well-recognized physiological reduction in spontaneous GH secretion with advancing age (142). It is therefore appropriate to consider older hypopituitary patients for GH replacement and to apply similar criteria to those outlined above. Elderly people with GH deficiency, in particular women, require less GH than at their earlier age, since they will be either spontaneously postmenopausal or taken off estrogen replacement.
TRANSITION BETWEEN PEDIATRIC AND ADULT CARE FOR CHILDHOOD ONSET GH DEFICIENCY
The transition from childhood into adulthood is generally a very vulnerable period in any young person’s life. It is therefore pertinent to make the transition as smooth as possible. The best way to do this is to have common transition clinics with both a pediatrician and adult endocrinologist having joint consultations to prepare the adolescent for what is going to happen. The timing can be somewhat individual but aiming at a time around final height and completion of puberty seems appropriate. The pediatrician should prepare the child for this/these consultation(s), and the adult endocrinologist taking over future follow up needs to be aware of the fact that obtaining final height and a post pubertal state does not mean that the adolescent is fully matured in a physiological as well as psychological sense.
It is important to confirm persistence of GH deficiency at the time of completion of linear growth, particularly in children with isolated GH deficiency (18). In the presence of a structural lesion in childhood and multiple hormone deficiencies or some genetic causes, a low IGF-I (in the absence of poorly controlled diabetes, liver disease, or oral estrogen) is sufficient to confirm GH deficiency, without a stimulation test (19). Subsequently, decisions must be taken regarding recommencement of GH or longitudinal clinical observation off treatment. Arguments supporting continuation of GH therapy include the observation of increased accumulation of fat mass off treatment (204, 205) and continued acquisition of bone mass in young adults continuing GH in contrast to static bone mass in those discontinuing treatment at the time of completion of linear growth (206). There is no detriment seen in QoL in those patients who withdraw from GH at the completion of linear growth. There is an apparent improvement in insulin sensitivity but, as is the case during normal puberty, this may not be beneficial in the context of continuing somatic development. Given that the major indication for adult GH replacement is the impairment of QOL, then there is no clear consensus as to which patients should continue therapy seamlessly, virtually without interruption, and in which patients it may be reasonable to undertake a period of careful clinical assessment. A recent observational study has raised concern about discontinuation of GH replacement therapy in pediatrics in severely persistent GH deficiency patients, as well as about the often insufficient dose of GH in the treatment of adult patients (207). Follow-up showed improvement in lipid profile and bone mineral density in severely persistent GH deficiency patients under GH therapy. In multivariate analysis, the associated pituitary deficits seemed stronger determinant factors of metabolic and bone status than GH deficiency per se. A consensus meeting convened by The European Society for Pediatric Endocrinology suggested offering continuation of therapy (after retesting) and monitoring those who decline continuation of treatment. If therapy is continued the optimum dosing strategy has not been clearly defined although a titration approach as outlined above would seem empirically appropriate (208). The Endocrine Society Clinical practice guidelines recommend GH therapy to be continued after adult height to allow full skeletal and muscle maturation, which is often delayed in this population (18, 19).
INTERACTIONS WITH OTHER PITUITARY AND ADRENAL HORMONES
GH is known to inhibit 11ßHSD-1, therefore favoring metabolism to inactive cortisone over active cortisol (72). Hence patients who are partially ACTH deficient or on suboptimal replacement should be carefully monitored at initiation of GH replacement, which might otherwise lead to partial cortisol deficiency, and risk of Addisonian crisis by even simple infections (118, 209).
GH also interacts with the TSH axis (120, 123). Patients without defined TSH deficiency demonstrate a reduction in serum thyroxine (T4) after initiation of GH replacement, although maintain stable serum liothyronine (T3) (10, 210, 211), and patients on thyroxine replacement frequently require an increase in their dose (120, 121, 212).The mechanism remains unclear, but it has been postulated that GH may enhance peripheral conversion of T4 to T3 but also have a central inhibitory effect on TSH release at least in children. Clinicians should therefore be aware that the hypothalamo-pituitary-thyroid axis can very easily be both underdiagnosed and under replaced in GH deficiency, and upon commencement of GH preplacement (120, 121, 213).
Women require a higher GH dose than men to achieve a similar increment in IGF-I. GH sensitivity is blunted in females on oral estrogen (214-216). Transdermal estrogen reduces IGF-I generation to a lesser extent than oral estrogen. The effect of estrogen is thought to be mainly due to first pass metabolism inhibiting hepatic synthesis of IGF-I (217, 218). Testosterone stimulates GH secretion centrally, and also amplifies GH stimulation of IGF-I (216, 217). In addition to gonadal steroids, DHEA replacement has been shown to have an impact on IGF-I generation and psychological well-being (219, 220). DHEA improves psychological well-being independently of an effect on IGF-I (229). DHEA has been shown to potentiate IGF-I generation (219, 220) such that females on DHEA replacement require a lower GH dose to achieve the same IGF-I (219, 221). The mechanism is unknown, but DHEA is metabolized to testosterone and it is postulated that increased serum testosterone may be responsible, hence explaining the lack of a DHEA effect in men who are either eugonadal or are on testosterone replacement.
GROWTH HORMONE REPLACEMENT
Selecting Patients for Growth Hormone Replacement
The diagnosis of GH deficiency in adults is usually straightforward and consensus guidelines have been established with generalized acceptance (Fig 8). Nonetheless there is continuing debate regarding the selection of patients for GH replacement. Practice varies between countries and is undoubtedly influenced by availability of funding for treatment. In clinical practice, patients are selected for treatment on the basis of perceived need according to one or more of a number of specific criteria as outlined in Tables 3 and 4, including severe GH deficiency defined by the insulin tolerance test (ITT), glucagon test or alternative tests such as arginine plus growth hormone releasing hormone (GHRH) or the Macimorellin test.
Establishing the Maintenance GH Dose
When the indication for GH-replacement has been ascertained, the patient is usually on a low initial dose (0.2 mg daily), but dependent on age, since adolescents during transition may benefit from higher initial doses, as will also women on estrogen therapy (replacement or oral contraceptives) a higher dose may be employed (214, 222-224). The dose titration is monitored by IGF-I concentrations (12, 154, 158), and a number of end organ end responses, which may act as ‘biomarkers’ of the treatment effects (table 6).
The doses used in published studies vary widely and much of the published data in this area is derived from dosing schedules established on body weight or surface area criteria which were in effect an extrapolation of earlier pediatric practice. Ongoing assessment in the routine clinical setting has indicated that patients can now be managed on much lower doses (158). Using a widely accepted clinical strategy, patients are commenced on 0.2 mg somatotrophin subcutaneously once a day initially. The dose is reviewed every two to four weeks according to clinical response, serum IGF-I levels, and any side effects and the dose is increased, if necessary, at 4 weekly intervals until the maintenance level is achieved (225). This results in a median dose requirement of 0.4 mg daily with a greater sensitivity to a given dose in male patients so that median dose requirement is lower in men. Several sustained release long-acting GH preparations are currently undergoing clinical trials (226-230) and may become an alternative, with some now being marketed in Asia, US and Europe. However, long-term surveillance of safety and efficacy of long-acting GH analogs are not available to address potential pitfalls of the sustained release preparations (231). Serum IGF-I levels may be in the lower part of the age-related reference range in approximately 40% of patients with adult-onset hypopituitarism before any GH treatment across the total age range and this becomes more likely with advancing age. An empirical strategy is to use the minimum dose of GH, which places the serum IGF-1 level between the median value and the upper limit of the age matched normal range for the individual patient. This approach minimizes the risk of overtreatment and the potential sequelae, which may ensue. Serum IGF binding protein-3 and acid-labile subunit lack sensitivity for the titration of GH replacement and are not recommended for this purpose. IGF-I, however, is regulated by several other factors than GH and changes in body composition can be seen with the addition of GH even without any alteration in the IGF-I level. For this reason other biomarkers of GH action are being sought (232).
Table 6.
What variables and organ functions should be followed in diagnosed GH deficient adult patients treated with GH replacement?
| Variables IGF-I (therapy monitoring, titrate to concentration between 0 and + 2SDS) Other pituitary hormone deficiencies MR/CT scan of pituitary in if abnormalities present Safety (adverse effect) QoL assessment (AGHDA) Metabolic variables Glucose metabolism Lipids BMI Body composition (waist-hip, fat mass, lean body mass) Dexa scan of bones Physical capacity Cardiovascular |
IGF-I: Insulin like Growth factor-I; MR: Magnetic Resonance; CT: Computer Tomography; QoL: Quality of Life; AGHDA: Adult growth hormone deficiency assessment: BMI: Body mass index
Adverse Effects
The main adverse effects directly attributable to GH replacement result from the correction of the sodium and water depletion present in GH deficiency patients. This manifests as arthralgia, myalgia, edema, and carpal tunnel syndrome and are usually rapidly reversible with GH dose reduction. They were predominantly a feature of the early experience when GH dose was determined by body weight rather than being based on a titration regimen commencing with a low starting dose as described above. Such adverse effects were predictably more frequent in male patients reflecting their greater sensitivity to GH. Benign intracranial hypertension is a recognized complication of GH replacement in pediatric practice but is much less likely in adult patients especially when low doses are used. However, persistent severe headache should prompt examination and investigation to exclude raised intracranial pressure. The potential mitogenic effects of IGF-I have raised concerns regarding a possible increased risk of either neoplasia or regrowth of residual pituitary and peripituitary tumors. Extensive surveillance studies based on large multinational databases, including several thousand patients on GH replacement followed longitudinally, have not demonstrated an increased incidence of de novo neoplasia and prospective magnetic resonance imaging studies have not indicated an increased risk of pituitary or parasellar tumor regrowth (233, 234). In the childhood cancer survivor study (235) there was no increased risk of recurrence over 5 years follow-up in those who received GH and on 15-year follow-up of patients with previous cranial irradiation who receive GH replacement there was no increased risk of malignancy (236). In addition, there has been no correlation between the serum IGF-I level within the normal reference range and risk of further malignancy (237).
Mortality
Definition of the precise relationship between GH deficiency and mortality must await long term observations of mortality rate in patients on GH replacement set against background mortality rates in the general population adjusted for national variations but a recent Dutch study provides some evidence that mortality is not increased by replacement and may play a role in normalizing it (particularly in men) (238).

The potential impact of GH replacement on the increased mortality rates described in hypopituitary patients can only be determined by long-term surveillance of treated patients in comparison with normal population data. The multinational databases designed to monitor safety of long-term GH replacement may provide useful information in this regard. Reassuringly, the mortality rates in the KIMS database were similar to the background populations (fig 18), and a later large study in a much larger population with longer follow-up did not observe any increased mortality in GH treated GH deficient patients in the KIMS database (26). Danish nationwide studies have indicated that mortality was not increased in GH treated patients with childhood onset GH deficiency (239, 240), but was highly dependent on the primary cause of GH deficiency (241), since the primary causes of childhood onset GH deficiency and concomitant diseases severely impaired socioeconomic conditions and impacted mortality; and only the subgroup of patients with idiopathic GH deficiency conditions was similar to the background population. In two Swedish publications there was evidence that hypocortisolism during acute stress, and de novo malignant brain tumors contributed to increased mortality (242), and GH deficient men receiving GH treatment had a mortality rate no different from the background population. In women, after exclusion of high-risk patients, mortality was not different from the background population except for CVD. Mortality due to malignancies was not elevated in adults receiving GH treatment. Next to gender, the heterogeneous etiology influences mortality in GH deficient adults with GH treatment (243). In the French SAGhE study mortality rates were increased in their population of adults treated as children with recombinant GH, particularly in those who had received the highest doses. Specific effects were detected in terms of death due to bone tumors or cerebral hemorrhage but not for all cancers. These results highlight the need for additional studies of long-term mortality and morbidity after GH treatment in childhood (244). Thus, the more recent studies have been reassuring concerning GH replacement and mortality, since those groups with higher mortality seem to have been limited to patient groups with a prior higher risk due to concomitant confounding mortality risks.
COSTS VERSUS BENEFITS OF GH REPLACEMENT THERAPY
Population studies in Sweden have documented a significantly greater medical and social burden for patients with established hypopituitarism. This continuing cost occurs irrespective of the initial cost of treating the pituitary pathology and derives from issues including unemployment, early retirement, depressive illness, and requirement for disability pension. A social circumstances analysis of the KIMS database has shown that approximately 11% of males and 31% of females require assistance with activities of daily living (245) (fig 19). Additional treatment cost factors, which might be inferred from risk factor profiles in adult GH deficiency populations, include increased prevalence of ischemic heart disease and increased fracture rates. So, whilst the cost of GH replacement to the hypopituitary population is easily determined, matching this with data for economic benefit requires a quantification of long-term complications arising from surrogate markers for long-term morbidity observed in GH deficient patients. Assessments of the effectiveness of GH replacement over time is influenced by the changing characteristics of the patients, with lower doses of GH replacement being used and a shorter period of time from diagnosis of GH deficiency to treatment (181). This means that accurate assessments of cost benefit using long-term data is not yet possible, and probably never will be. A recent study based on patients enrolled into the KIMS database has demonstrated significant reductions in the numbers of patients requiring assistance with the activities of daily living, a decrease in medical consultations and a decrease in hospital in-patient stays over a period of 24 months of GH replacement (fig 20).

Fig 19.
Activity of daily living in adult patient with GH deficiency before and after GH replacement therapy. From: Hernberg-Stahl et al (245)

Fig 20.
Sick leave and length of hospital stays in adult patients with GH deficiency before and after GH replacement therapy. From: Hernberg-Stahl et al (245).
ADHERENCE TO MANAGEMENT OF ADULT GROWTH HORMONE DEFICIENCY IN CLINICAL PRACTICE
Despite 30 years of evidence, guidelines, and clinical experience with adult GH deficiency and its management, a very recently published survey within the auspices of European Society of Endocrinology (246) has indicated that despite many guidelines on safety and efficacy of GH replacement in deficient patients as well as the above health economic considerations, GH replacement is still not available or reimbursed in all European countries. It also seems that both health care professionals and health administrators need improved knowledge to optimize the care of adults with GH deficiency. The publication results were further commented upon (247) indicating that in some health care communities reimbursement has been a major issue, because the discussion of GH replacement in truly GH deficient adults has been mixed with the discussion of utilizing GH therapy for sporting enhancement or for anti-ageing purposes, both of which are strongly discouraged. Also continuous presentations of unclear indications for GH diagnosis and replacement in small cohorts of mixed etiologies also pollute the field of health care discussions of proper clear cut cases of GH deficiency according to the official guidelines (248).
REFERENCES
- 1.
- Cushing H. The Pituitary Body and its Disorders: Clinical States produced by Disorders of the Hypophysis Cerebri. The Journal of Laryngology, Rhinology, and Otology. 1913;28(7):382–90.
- 2.
- Raben MS. Growth hormone. 2. Clinical use of human growth hormone. N Engl J Med. 1962;266:82-6 concl. [PubMed: 14489585]
- 3.
- Utiger RD, Parker ML, Daughaday WH. Studies on human growth hormone. I. A radio-immunoassay for human growth hormone. The Journal of clinical investigation. 1962;41(2):254–61. [PMC free article: PMC289221] [PubMed: 13924012]
- 4.
- Jorgensen JO, Pedersen SA, Thuesen L, Jorgensen J, Ingemann-Hansen T, Skakkebaek NE, et al. Beneficial effects of growth hormone treatment in GH-deficient adults. Lancet. 1989;1(8649):1221–5. [PubMed: 2566779]
- 5.
- Salomon F, Cuneo RC, Hesp R, Sonksen PH. The effects of treatment with recombinant human growth hormone on body composition and metabolism in adults with growth hormone deficiency. NEnglJMed. 1989;321(26):1797–803. [PubMed: 2687691]
- 6.
- Cuneo RC, Salomon F, McGauley GA, Sönksen PH. The growth hormone deficiency syndrome in adults. Clin Endocrinol (Oxf). 1992;37(5):387–97. [PubMed: 1486686]
- 7.
- de Boer H, Blok GJ, Van der Veen EA. Clinical aspects of growth hormone deficiency in adults. Endocrine reviews. 1995;16(1):63–86. [PubMed: 7758433]
- 8.
- Carroll PV, Christ ER, Bengtsson BA, Carlsson L, Christiansen JS, Clemmons D, et al. Growth hormone deficiency in adulthood and the effects of growth hormone replacement: a review. Growth Hormone Research Society Scientific Committee. The Journal of Clinical Endocrinology and Metabolism. 1998;83(2):382–95. [PubMed: 9467546]
- 9.
- Littley MD, Shalet SM, Beardwell CG, Ahmed SR, Applegate G, Sutton ML. Hypopituitarism following external radiotherapy for pituitary tumours in adults. The Quarterly journal of medicine. 1989;70(262):145–60. [PubMed: 2594955]
- 10.
- Feldt-Rasmussen U, Klose M. Central hypothyroidism and its role for cardiovascular risk factors in hypopituitary patients. Endocrine. 2016;54(1):15–23. [PubMed: 27481361]
- 11.
- Consensus guidelines for the diagnosis and treatment of adults with growth hormone deficiency: summary statement of the Growth Hormone Research Society Workshop on Adult Growth Hormone Deficiency. The Journal of Clinical Endocrinology and Metabolism. 1998;83(2):379–81. [PubMed: 9467545]
- 12.
- Ho KK. Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. European Journal of Endocrinology. 2007;157(6):695–700. [PubMed: 18057375]
- 13.
- Ho KY, Hoffman DM. Growth hormone replacement therapy in adults – pros and cons. Larsson C, Butenandt O, editors. Tel Aviv/London: Freund Publishing House; 1993.
- 14.
- Höybye C, Beck-Peccoz P, Simsek S, Zabransky M, Zouater H, Stalla G, et al. Safety of current recombinant human growth hormone treatments for adults with growth hormone deficiency and unmet needs. Expert opinion on drug safety. 2020;19(12):1539–48. [PubMed: 33089723]
- 15.
- Webb SM, Strasburger CJ, Mo D, Hartman ML, Melmed S, Jung H, et al. Changing patterns of the adult growth hormone deficiency diagnosis documented in a decade-long global surveillance database. J Clin Endocrinol Metab. 2009;94(2):392–9. [PubMed: 19001512]
- 16.
- Höybye C, Burman P, Feldt-Rasmussen U, Hey-Hadavi J, Aydin F, Camacho-Hubner C, et al. Change in baseline characteristics over 20 years of adults with growth hormone (GH) deficiency on GH replacement therapy. Eur J Endocrinol. 2019;181(6):629–38. [PubMed: 31590143]
- 17.
- Klose M, Feldt-Rasmussen U. Chronic endocrine consequences of traumatic brain injury - what is the evidence? Nature reviews Endocrinology. 2018;14(1):57–62. [PubMed: 28885623]
- 18.
- Yuen KCJ, Biller BMK, Radovick S, Carmichael JD, Jasim S, Pantalone KM, et al. AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY GUIDELINES FOR MANAGEMENT OF GROWTH HORMONE DEFICIENCY IN ADULTS AND PATIENTS TRANSITIONING FROM PEDIATRIC TO ADULT CARE. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2019;25(11):1191-232. [PubMed: 31760824]
- 19.
- Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML. Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology and Metabolism. 2011;96(6):1587–609. [PubMed: 21602453]
- 20.
- Fernandez A, Karavitaki N, Wass JA. Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol (Oxf). 2010;72(3):377–82. [PubMed: 19650784]
- 21.
- Agustsson TT, Baldvinsdottir T, Jonasson JG, Olafsdottir E, Steinthorsdottir V, Sigurdsson G, et al. The epidemiology of pituitary adenomas in Iceland, 1955-2012: a nationwide population-based study. Eur J Endocrinol. 2015;173(5):655–64. [PubMed: 26423473]
- 22.
- Daly AF, Beckers A. The Epidemiology of Pituitary Adenomas. Endocrinology and metabolism clinics of North America. 2020;49(3):347–55. [PubMed: 32741475]
- 23.
- Stochholm K, Gravholt CH, Laursen T, Jorgensen JO, Laurberg P, Andersen M, et al. Incidence of GH deficiency - a nationwide study. European Journal of Endocrinology. 2006;155(1):61–71. [PubMed: 16793951]
- 24.
- Parkin JM. Incidence of growth hormone deficiency. Archives of disease in childhood. 1974;49(11):904–5. [PMC free article: PMC1649242] [PubMed: 4441124]
- 25.
- Sassolas G, Chazot FB, Jaquet P, Bachelot I, Chanson P, Rudelli CC, et al. GH deficiency in adults: an epidemiological approach. Eur J Endocrinol. 1999;141(6):595–600. [PubMed: 10601962]
- 26.
- Gaillard RC, Mattsson AF, Akerblad AC, Bengtsson B, Cara J, Feldt-Rasmussen U, et al. Overall and cause-specific mortality in GH-deficient adults on GH replacement. Eur J Endocrinol. 2012;166(6):1069–77. [PubMed: 22457236]
- 27.
- Klose M, Feldt-Rasmussen U. Hypopituitarism in Traumatic Brain Injury-A Critical Note. Journal of clinical medicine. 2015;4(7):1480–97. [PMC free article: PMC4519801] [PubMed: 26239687]
- 28.
- Klose M, Stochholm K, Janukonyte J, Lehman CL, Frystyk J, Andersen M, et al. Prevalence of posttraumatic growth hormone deficiency is highly dependent on the diagnostic set-up: results from The Danish National Study on Posttraumatic Hypopituitarism. The Journal of Clinical Endocrinology and Metabolism. 2014;99(1):101–10. [PubMed: 24243629]
- 29.
- Barroso-Sousa R, Barry WT, Garrido-Castro AC, Hodi FS, Min L, Krop IE, et al. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA oncology. 2018;4(2):173–82. [PMC free article: PMC5838579] [PubMed: 28973656]
- 30.
- Torino F, Barnabei A, Paragliola RM, Marchetti P, Salvatori R, Corsello SM. Endocrine side-effects of anti-cancer drugs: mAbs and pituitary dysfunction: clinical evidence and pathogenic hypotheses. Eur J Endocrinol. 2013;169(6):R153–64. [PubMed: 24001893]
- 31.
- Gleeson HK, Gattamaneni HR, Smethurst L, Brennan BM, Shalet SM. Reassessment of growth hormone status is required at final height in children treated with growth hormone replacement after radiation therapy. J Clin Endocrinol Metab. 2004;89(2):662–6. [PubMed: 14764778]
- 32.
- Gasco V, Corneli G, Beccuti G, Prodam F, Rovere S, Bellone J, et al. Retesting the childhood-onset GH-deficient patient. Eur J Endocrinol. 2008;159 Suppl 1:S45–52. [PubMed: 18805914]
- 33.
- Berberoğlu M, Sıklar Z, Darendeliler F, Poyrazoğlu S, Darcan S, Işgüven P, et al. Evaluation of permanent growth hormone deficiency (GHD) in young adults with childhood onset GHD: a multicenter study. Journal of clinical research in pediatric endocrinology. 2008;1(1):30–7. [PMC free article: PMC3005632] [PubMed: 21318062]
- 34.
- Rasmussen MH, Hvidberg A, Juul A, Main KM, Gotfredsen A, Skakkebaek NE, et al. Massive weight loss restores 24-hour growth hormone release profiles and serum insulin-like growth factor-I levels in obese subjects. The Journal of Clinical Endocrinology and Metabolism. 1995;80(4):1407–15. [PubMed: 7536210]
- 35.
- De Marinis L, Bianchi A, Mancini A, Gentilella R, Perrelli M, Giampietro A, et al. Growth hormone secretion and leptin in morbid obesity before and after biliopancreatic diversion: relationships with insulin and body composition. J Clin Endocrinol Metab. 2004;89(1):174–80. [PubMed: 14715846]
- 36.
- Makimura H, Stanley T, Mun D, You SM, Grinspoon S. The effects of central adiposity on growth hormone (GH) response to GH-releasing hormone-arginine stimulation testing in men. The Journal of Clinical Endocrinology and Metabolism. 2008;93(11):4254–60. [PMC free article: PMC2582562] [PubMed: 18765508]
- 37.
- Rasmussen MH. Obesity, growth hormone and weight loss. Molecular and cellular endocrinology. 2010;316(2):147–53. [PubMed: 19723558]
- 38.
- Klose M, Jonsson B, Abs R, Popovic V, Koltowska-Häggström M, Saller B, et al. From isolated GH deficiency to multiple pituitary hormone deficiency: an evolving continuum - a KIMS analysis. Eur J Endocrinol. 2009;161 Suppl 1:S75–83. [PubMed: 19684053]
- 39.
- Blum WF, Deal C, Zimmermann AG, Shavrikova EP, Child CJ, Quigley CA, et al. Development of additional pituitary hormone deficiencies in pediatric patients originally diagnosed with idiopathic isolated GH deficiency. Eur J Endocrinol. 2014;170(1):13–21. [PubMed: 24088548]
- 40.
- Child CJ, Blum WF, Deal C, Zimmermann AG, Quigley CA, Drop SL, et al. Development of additional pituitary hormone deficiencies in pediatric patients originally diagnosed with isolated growth hormone deficiency due to organic causes. Eur J Endocrinol. 2016;174(5):669–79. [PubMed: 26888628]
- 41.
- Arafah BM, Kailani SH, Nekl KE, Gold RS, Selman WR. Immediate recovery of pituitary function after transsphenoidal resection of pituitary macroadenomas. The Journal of Clinical Endocrinology and Metabolism. 1994;79(2):348–54. [PubMed: 8045946]
- 42.
- Fatemi N, Dusick JR, Mattozo C, McArthur DL, Cohan P, Boscardin J, et al. Pituitary hormonal loss and recovery after transsphenoidal adenoma removal. Neurosurgery. 2008;63(4):709–18. [PubMed: 18981881]
- 43.
- Pedersen MB, Dukanovic S, Springborg JB, Andreassen M, Krogh J. Endocrine function after transsphenoidal surgery in patients with non-functioning pituitary adenomas: A systematic review and meta-analysis. Neuroendocrinology. 2022 [PubMed: 35172314]
- 44.
- Jørgensen JO, Müller J, Møller J, Wolthers T, Vahl N, Juul A, et al. Adult growth hormone deficiency. Hormone research. 1994;42(4-5):235–41. [PubMed: 7868079]
- 45.
- Weaver JU, Monson JP, Noonan K, John WG, Edwards A, Evans KA, et al. The effect of low dose recombinant human growth hormone replacement on regional fat distribution, insulin sensitivity, and cardiovascular risk factors in hypopituitary adults. J Clin Endocrinol Metab. 1995;80(1):153–9. [PubMed: 7829604]
- 46.
- Rosén T, Bosaeus I, Tölli J, Lindstedt G, Bengtsson BA. Increased body fat mass and decreased extracellular fluid volume in adults with growth hormone deficiency. Clin Endocrinol (Oxf). 1993;38(1):63–71. [PubMed: 8435887]
- 47.
- Li Voon Chong JS, Groves T, Foy P, Wallymahmed ME, MacFarlane IA. Elderly people with hypothalamic-pituitary disease and untreated GH deficiency: clinical outcome, body composition, lipid profiles and quality of life after 2 years compared to controls. Clin Endocrinol (Oxf). 2002;56(2):175–81. [PubMed: 11874408]
- 48.
- Bengtsson BA, Abs R, Bennmarker H, Monson JP, Feldt-Rasmussen U, Hernberg-Stahl E, et al. The effects of treatment and the individual responsiveness to growth hormone (GH) replacement therapy in 665 GH-deficient adults. KIMS Study Group and the KIMS International Board. J Clin Endocrinol Metab. 1999;84(11):3929–35. [PubMed: 10566630]
- 49.
- Gomes-Santos E, Salvatori R, Ferrão TO, Oliveira CR, Diniz RD, Santana JA, et al. Increased visceral adiposity and cortisol to cortisone ratio in adults with congenital lifetime isolated GH deficiency. J Clin Endocrinol Metab. 2014;99(9):3285–9. [PubMed: 24926956]
- 50.
- Fideleff HL, Boquete HR, Stalldecker G, Giaccio AV, Sobrado PG. Comparative results of a 4-year study on cardiovascular parameters, lipid metabolism, body composition and bone mass between untreated and treated adult growth hormone deficient patients. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2008;18(4):318-24. [PubMed: 18289903]
- 51.
- Mersebach H, Feldt-Rasmussen U. Growth hormone and body composition. Frontiers of hormone research. 2005;33:185–95. [PubMed: 16166762]
- 52.
- Feldt-Rasmussen U, Wilton P, Jonsson P. Aspects of growth hormone deficiency and replacement in elderly hypopituitary adults. Growth HormIGFRes. 2004;14 Suppl A:S51-S8. [PubMed: 15135778]
- 53.
- Drake WM, Rodríguez-Arnao J, Weaver JU, James IT, Coyte D, Spector TD, et al. The influence of gender on the short and long-term effects of growth hormone replacement on bone metabolism and bone mineral density in hypopituitary adults: a 5-year study. Clin Endocrinol (Oxf). 2001;54(4):525–32. [PubMed: 11318789]
- 54.
- Johansson JO, Landin K, Tengborn L, Rosén T, Bengtsson BA. High fibrinogen and plasminogen activator inhibitor activity in growth hormone-deficient adults. Arteriosclerosis and thrombosis : a journal of vascular biology. 1994;14(3):434-7. [PubMed: 8123648]
- 55.
- Klose M, Watt T, Brennum J, Feldt-Rasmussen U. Posttraumatic hypopituitarism is associated with an unfavorable body composition and lipid profile, and decreased quality of life 12 months after injury. The Journal of Clinical Endocrinology and Metabolism. 2007;92(10):3861–8. [PubMed: 17652217]
- 56.
- Abs R, Mattsson AF, Bengtsson BA, Feldt-Rasmussen U, Goth MI, Koltowska-Haggstrom M, et al. Isolated growth hormone (GH) deficiency in adult patients: baseline clinical characteristics and responses to GH replacement in comparison with hypopituitary patients. A sub-analysis of the KIMS database. Growth HormIGFRes. 2005;15(5):349–59. [PubMed: 16168692]
- 57.
- Merola B, Sofia M, Longobardi S, Fazio S, Micco A, Esposito V, et al. Impairment of lung volumes and respiratory muscle strength in adult patients with growth hormone deficiency. Eur J Endocrinol. 1995;133(6):680–5. [PubMed: 8548052]
- 58.
- Janssen YJ, Doornbos J, Roelfsema F. Changes in muscle volume, strength, and bioenergetics during recombinant human growth hormone (GH) therapy in adults with GH deficiency. J Clin Endocrinol Metab. 1999;84(1):279–84. [PubMed: 9920096]
- 59.
- Modesto Mde J, Amer NM, Erichsen O, Hernandez S, dos Santos CD, de Carvalho J, et al. Muscle strength and body composition during the transition phase in patients treated with recombinant GH to final height. Journal of pediatric endocrinology & metabolism. JPEM. 2014;27(9-10):813–20. [PubMed: 24756044]
- 60.
- Johannsson G, Sverrisdóttir YB, Ellegård L, Lundberg PA, Herlitz H. GH increases extracellular volume by stimulating sodium reabsorption in the distal nephron and preventing pressure natriuresis. J Clin Endocrinol Metab. 2002;87(4):1743–9. [PubMed: 11932310]
- 61.
- Simpson JA, Lobo DN, Anderson JA, Macdonald IA, Perkins AC, Neal KR, et al. Body water compartment measurements: a comparison of bioelectrical impedance analysis with tritium and sodium bromide dilution techniques. Clinical nutrition (Edinburgh, Scotland). 2001;20(4):339-43. [PubMed: 11478832]
- 62.
- Møller J, Frandsen E, Fisker S, Jørgensen JO, Christiansen JS. Decreased plasma and extracellular volume in growth hormone deficient adults and the acute and prolonged effects of GH administration: a controlled experimental study. Clin Endocrinol (Oxf). 1996;44(5):533–9. [PubMed: 8762729]
- 63.
- Jørgensen JO, Vahl N, Hansen TB, Thuesen L, Hagen C, Christiansen JS. Growth hormone versus placebo treatment for one year in growth hormone deficient adults: increase in exercise capacity and normalization of body composition. Clin Endocrinol (Oxf). 1996;45(6):681–8. [PubMed: 9039333]
- 64.
- Widdowson WM, Gibney J. The effect of growth hormone replacement on exercise capacity in patients with GH deficiency: a metaanalysis. J Clin Endocrinol Metab. 2008;93(11):4413–7. [PubMed: 18697875]
- 65.
- Lombardi G, Colao A, Cuocolo A, Longobardi S, Di Somma C, Orio F, et al. Cardiological aspects of growth hormone and insulin-like growth factor-I. Journal of pediatric endocrinology & metabolism. JPEM. 1997;10(6):553–60. [PubMed: 9467124]
- 66.
- Colao A, Cuocolo A, Di Somma C, Cerbone G, Della Morte AM, Nicolai E, et al. Impaired cardiac performance in elderly patients with growth hormone deficiency. J Clin Endocrinol Metab. 1999;84(11):3950–5. [PubMed: 10566633]
- 67.
- Thuesen L, Jørgensen JO, Müller JR, Kristensen BO, Skakkebaek NE, Vahl N, et al. Short and long-term cardiovascular effects of growth hormone therapy in growth hormone deficient adults. Clin Endocrinol (Oxf). 1994;41(5):615–20. [PubMed: 7828351]
- 68.
- Lanes R, Gunczler P, Lopez E, Esaa S, Villaroel O, Revel-Chion R. Cardiac mass and function, carotid artery intima-media thickness, and lipoprotein levels in growth hormone-deficient adolescents. J Clin Endocrinol Metab. 2001;86(3):1061–5. [PubMed: 11238486]
- 69.
- Maison P, Chanson P. Cardiac effects of growth hormone in adults with growth hormone deficiency: a meta-analysis. Circulation. 2003;108(21):2648–52. [PubMed: 14623813]
- 70.
- Moisey R, Orme S, Barker D, Lewis N, Sharp L, Clements RE, et al. Cardiac functional reserve is diminished in growth hormone-deficient adults. Cardiovascular therapeutics. 2009;27(1):34–41. [PubMed: 19207478]
- 71.
- Thomas JD, Dattani A, Zemrak F, Burchell T, Akker SA, Gurnell M, et al. Characterisation of myocardial structure and function in adult-onset growth hormone deficiency using cardiac magnetic resonance. Endocrine. 2016;54(3):778–87. [PMC free article: PMC5107200] [PubMed: 27535681]
- 72.
- Mihaila S, Mincu RI, Rimbas RC, Dulgheru RE, Dobrescu R, Magda SL, et al. Growth hormone deficiency in adults impacts left ventricular mechanics: a two-dimensional speckle-tracking study. The Canadian journal of cardiology. 2015;31(6):752–9. [PubMed: 26022988]
- 73.
- Sneppen SB, Steensgaard-Hansen F, Feldt-Rasmussen U. Cardiac effects of low-dose growth hormone replacement therapy in growth hormone-deficient adults. An 18-month randomised, placebo-controlled, double-blind study. Hormone research. 2002;58(1):21–9. [PubMed: 12169777]
- 74.
- Andreassen M, Faber J, Kjaer A, Petersen CL, Kristensen L. Cardiac function in growth hormone deficient patients before and after 1 year with replacement therapy: a magnetic resonance imaging study. Pituitary. 2011;14(1):1–10. [PubMed: 20730514]
- 75.
- Ozdogru I, Tanriverdi F, Dogan A, Kaya MG, Tugrul Inanc M, Kalay N, et al. Impaired longitudinal myocardial velocities in patients with growth hormone deficiency improves after hormone replacement therapy. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2007;20(9):1093–9. [PubMed: 17555934]
- 76.
- Jørgensen JO, Krag M, Jessen N, Nørrelund H, Vestergaard ET, Møller N, et al. Growth hormone and glucose homeostasis. Hormone research. 2004;62 Suppl 3:51–5. [PubMed: 15539799]
- 77.
- Fowelin J, Attvall S, Lager I, Bengtsson BA. Effects of treatment with recombinant human growth hormone on insulin sensitivity and glucose metabolism in adults with growth hormone deficiency. Metabolism. 1993;42(11):1443–7. [PubMed: 8231841]
- 78.
- Giovannini L, Tirabassi G, Muscogiuri G, Di Somma C, Colao A, Balercia G. Impact of adult growth hormone deficiency on metabolic profile and cardiovascular risk. Endocrine journal. 2015;62(12):1037–48. [Review] [PubMed: 26300280]
- 79.
- Oliveira CR, Salvatori R, Barreto-Filho JA, Rocha IE, Mari A, Pereira RM, et al. Insulin sensitivity and β-cell function in adults with lifetime, untreated isolated growth hormone deficiency. J Clin Endocrinol Metab. 2012;97(3):1013–9. [PubMed: 22170707]
- 80.
- Vicente TA, Rocha IE, Salvatori R, Oliveira CR, Pereira RM, Souza AH, et al. Lifetime congenital isolated GH deficiency does not protect from the development of diabetes. Endocrine connections. 2013;2(2):112–7. [PMC free article: PMC3689269] [PubMed: 23795286]
- 81.
- Gelding SV, Taylor NF, Wood PJ, Noonan K, Weaver JU, Wood DF, et al. The effect of growth hormone replacement therapy on cortisol-cortisone interconversion in hypopituitary adults: evidence for growth hormone modulation of extrarenal 11 beta-hydroxysteroid dehydrogenase activity. Clin Endocrinol (Oxf). 1998;48(2):153–62. [PubMed: 9579226]
- 82.
- Roemmler J, Kuenkler M, Schneider HJ, Dieterle C, Schopohl J. Comparison of glucose and lipid metabolism and bone mineralization in patients with growth hormone deficiency with and without long-term growth hormone replacement. Metabolism. 2010;59(3):350–8. [PubMed: 19800640]
- 83.
- Elbornsson M, Götherström G, Bosæus I, Bengtsson B, Johannsson G, Svensson J. Fifteen years of GH replacement improves body composition and cardiovascular risk factors. Eur J Endocrinol. 2013;168(5):745–53. [PMC free article: PMC3625369] [PubMed: 23428613]
- 84.
- Markussis V, Beshyah SA, Fisher C, Sharp P, Nicolaides AN, Johnston DG. Detection of premature atherosclerosis by high-resolution ultrasonography in symptom-free hypopituitary adults. Lancet. 1992;340(8829):1188–92. [PubMed: 1359261]
- 85.
- Capaldo B, Patti L, Oliviero U, Longobardi S, Pardo F, Vitale F, et al. Increased arterial intima-media thickness in childhood-onset growth hormone deficiency. J Clin Endocrinol Metab. 1997;82(5):1378–81. [PubMed: 9141519]
- 86.
- Johansson AG, Burman P, Westermark K, Ljunghall S. The bone mineral density in acquired growth hormone deficiency correlates with circulating levels of insulin-like growth factor I. Journal of internal medicine. 1992;232(5):447–52. [PubMed: 1453131]
- 87.
- Kaufman JM, Taelman P, Vermeulen A, Vandeweghe M. Bone mineral status in growth hormone-deficient males with isolated and multiple pituitary deficiencies of childhood onset. J Clin Endocrinol Metab. 1992;74(1):118–23. [PubMed: 1727808]
- 88.
- Bing-You RG, Denis MC, Rosen CJ. Low bone mineral density in adults with previous hypothalamic-pituitary tumors: correlations with serum growth hormone responses to GH-releasing hormone, insulin-like growth factor I, and IGF binding protein 3. Calcified tissue international. 1993;52(3):183–7. [PubMed: 7683247]
- 89.
- Rosén T, Hansson T, Granhed H, Szucs J, Bengtsson BA. Reduced bone mineral content in adult patients with growth hormone deficiency. Acta endocrinologica. 1993;129(3):201–6. [PubMed: 8212984]
- 90.
- de Boer H, Blok GJ, van Lingen A, Teule GJ, Lips P, van der Veen EA. Consequences of childhood-onset growth hormone deficiency for adult bone mass. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 1994;9(8):1319-26. [PubMed: 7976513]
- 91.
- Holmes SJ, Economou G, Whitehouse RW, Adams JE, Shalet SM. Reduced bone mineral density in patients with adult onset growth hormone deficiency. J Clin Endocrinol Metab. 1994;78(3):669–74. [PubMed: 8126140]
- 92.
- Wuster C, Abs R, Bengtsson BA, Bennmarker H, Feldt-Rasmussen U, Hernberg-Stahl E, et al. The influence of growth hormone deficiency, growth hormone replacement therapy, and other aspects of hypopituitarism on fracture rate and bone mineral density. JBone MinerRes. 2001;16(2):398–405. [PubMed: 11204440]
- 93.
- Vestergaard P, Jørgensen JO, Hagen C, Hoeck HC, Laurberg P, Rejnmark L, et al. Fracture risk is increased in patients with GH deficiency or untreated prolactinomas--a case-control study. Clin Endocrinol (Oxf). 2002;56(2):159–67. [PubMed: 11874406]
- 94.
- Mazziotti G, Doga M, Frara S, Maffezzoni F, Porcelli T, Cerri L, et al. Incidence of morphometric vertebral fractures in adult patients with growth hormone deficiency. Endocrine. 2016;52(1):103–10. [PubMed: 26433736]
- 95.
- Rosén T, Wilhelmsen L, Landin-Wilhelmsen K, Lappas G, Bengtsson BA. Increased fracture frequency in adult patients with hypopituitarism and GH deficiency. Eur J Endocrinol. 1997;137(3):240–5. [PubMed: 9330587]
- 96.
- Lange M, Müller J, Svendsen OL, Kastrup KW, Juul A, Feldt-Rasmussen U. The impact of idiopathic childhood-onset growth hormone deficiency (GHD) on bone mass in subjects without adult GHD. Clin Endocrinol (Oxf). 2005;62(1):18–23. [PubMed: 15638865]
- 97.
- Tritos NA, Greenspan SL, King D, Hamrahian A, Cook DM, Jönsson PJ, et al. Unreplaced sex steroid deficiency, corticotropin deficiency, and lower IGF-I are associated with lower bone mineral density in adults with growth hormone deficiency: a KIMS database analysis. J Clin Endocrinol Metab. 2011;96(5):1516–23. [PMC free article: PMC5393425] [PubMed: 21367928]
- 98.
- Mazziotti G, Porcelli T, Bianchi A, Cimino V, Patelli I, Mejia C, et al. Glucocorticoid replacement therapy and vertebral fractures in hypopituitary adult males with GH deficiency. Eur J Endocrinol. 2010;163(1):15–20. [PubMed: 20378720]
- 99.
- Feldt-Rasmussen U, Abs R, Bengtsson BA, Bennmarker H, Bramnert M, Hernberg-Ståhl E, et al. Growth hormone deficiency and replacement in hypopituitary patients previously treated for acromegaly or Cushing's disease. Eur J Endocrinol. 2002;146(1):67–74. [PubMed: 11751070]
- 100.
- Höybye C, Ragnarsson O, Jönsson PJ, Koltowska-Häggström M, Trainer P, Feldt-Rasmussen U, et al. Clinical features of GH deficiency and effects of 3 years of GH replacement in adults with controlled Cushing's disease. Eur J Endocrinol. 2010;162(4):677–84. [PubMed: 20089548]
- 101.
- Lange M, Qvortrup K, Svendsen OL, Flyvbjerg A, Nowak J, Petersen MM, et al. Abnormal bone collagen morphology and decreased bone strength in growth hormone-deficient rats. Bone. 2004;35(1):178–85. [PubMed: 15207754]
- 102.
- Doessing S, Holm L, Heinemeier KM, Feldt-Rasmussen U, Schjerling P, Qvortrup K, et al. GH and IGF1 levels are positively associated with musculotendinous collagen expression: experiments in acromegalic and GH deficiency patients. Eur J Endocrinol. 2010;163(6):853–62. [PubMed: 20858702]
- 103.
- https://www
.nice.org .uk/guidance/TA64?UNLID =10228138712014122893019?print=true. Human growth hormone (somatropin) in adults with growth hormone deficiency. 2017. - 104.
- Chikani V, Cuneo RC, Hickman I, Ho KK. Impairment of anaerobic capacity in adults with growth hormone deficiency. J Clin Endocrinol Metab. 2015;100(5):1811–8. [PubMed: 25695894]
- 105.
- Herschbach P, Henrich G, Strasburger CJ, Feldmeier H, Marín F, Attanasio AM, et al. Development and psychometric properties of a disease-specific quality of life questionnaire for adult patients with growth hormone deficiency. Eur J Endocrinol. 2001;145(3):255–65. [PubMed: 11517005]
- 106.
- Gilchrist FJ, Murray RD, Shalet SM. The effect of long-term untreated growth hormone deficiency (GHD) and 9 years of GH replacement on the quality of life (QoL) of GH-deficient adults. Clin Endocrinol (Oxf). 2002;57(3):363–70. [PubMed: 12201829]
- 107.
- McKenna SP, Doward LC, Alonso J, Kohlmann T, Niero M, Prieto L, et al. The QoL-AGHDA: an instrument for the assessment of quality of life in adults with growth hormone deficiency. QualLife Res. 1999;8(4):373–83. [PubMed: 10472170]
- 108.
- Wiren L, Whalley D, McKenna S, Wilhelmsen L. Application of a disease-specific, quality-of-life measure (QoL-AGHDA) in growth hormone-deficient adults and a random population sample in Sweden: validation of the measure by rasch analysis. Clinical Endocrinology. 2000;52(2):143–52. [PubMed: 10671940]
- 109.
- Koltowska-Haggstrom M, Hennessy S, Mattsson AF, Monson JP, Kind P. Quality of life assessment of growth hormone deficiency in adults (QoL-AGHDA): comparison of normative reference data for the general population of England and Wales with results for adult hypopituitary patients with growth hormone deficiency. HormRes. 2005;64(1):46–54. [PubMed: 16103683]
- 110.
- Webb SM. Measurements of quality of life in patients with growth hormone deficiency. Journal of endocrinological investigation. 2008;31(9) Suppl:52–5. [PubMed: 19020387]
- 111.
- Woodhouse LJ, Mukherjee A, Shalet SM, Ezzat S. The influence of growth hormone status on physical impairments, functional limitations, and health-related quality of life in adults. Endocrine reviews. 2006;27(3):287–317. [PubMed: 16543384]
- 112.
- Rosen T, Bengtsson BA. Premature mortality due to cardiovascular disease in hypopituitarism. Lancet. 1990;336(8710):285–8. [PubMed: 1973979]
- 113.
- Bülow B, Hagmar L, Mikoczy Z, Nordström CH, Erfurth EM. Increased cerebrovascular mortality in patients with hypopituitarism. Clin Endocrinol (Oxf). 1997;46(1):75–81. [PubMed: 9059561]
- 114.
- Tomlinson JW, Holden N, Hills RK, Wheatley K, Clayton RN, Bates AS, et al. Association between premature mortality and hypopituitarism. West Midlands Prospective Hypopituitary Study Group. Lancet. 2001;357(9254):425–31. [PubMed: 11273062]
- 115.
- Bates AS, Van't Hoff W, Jones PJ, Clayton RN. The effect of hypopituitarism on life expectancy. The Journal of Clinical Endocrinology and Metabolism. 1996;81(3):1169–72. [PubMed: 8772595]
- 116.
- Erfurth EM, Bülow B, Eskilsson J, Hagmar L. High incidence of cardiovascular disease and increased prevalence of cardiovascular risk factors in women with hypopituitarism not receiving growth hormone treatment: preliminary results. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 1999;9 Suppl A:21-4. [PubMed: 10429876]
- 117.
- Bengtsson BA. Untreated growth hormone deficiency explains premature mortality in patients with hypopituitarism. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 1998;8 Suppl A:77-80. [PubMed: 10993596]
- 118.
- Filipsson H, Monson JP, Koltowska-Haggstrom M, Mattsson A, Johannsson G. The impact of glucocorticoid replacement regimens on metabolic outcome and comorbidity in hypopituitary patients. J Clin Endocrinol Metab. 2006;91(10):3954–61. [PubMed: 16895963]
- 119.
- Ragnarsson O, Nyström HF, Johannsson G. Glucocorticoid replacement therapy is independently associated with reduced bone mineral density in women with hypopituitarism. Clin Endocrinol (Oxf). 2012;76(2):246–52. [PubMed: 21767286]
- 120.
- Filipsson Nyström H, Feldt-Rasmussen U, Kourides I, Popovic V, Koltowska-Häggström M, Jonsson B, et al. The metabolic consequences of thyroxine replacement in adult hypopituitary patients. Pituitary. 2012;15(4):495–504. [PubMed: 22038030]
- 121.
- Klose M, Marina D, Hartoft-Nielsen ML, Klefter O, Gavan V, Hilsted L, et al. Central hypothyroidism and its replacement have a significant influence on cardiovascular risk factors in adult hypopituitary patients. J Clin Endocrinol Metab. 2013;98(9):3802–10. [PubMed: 23796569]
- 122.
- Filipsson H, Johannsson G. GH replacement in adults: interactions with other pituitary hormone deficiencies and replacement therapies. Eur J Endocrinol. 2009;161 Suppl 1:S85–95. [PubMed: 19684055]
- 123.
- Feldt-Rasmussen U. Interactions between growth hormone and the thyroid gland -- with special reference to biochemical diagnosis. Current medicinal chemistry. 2007;14(26):2783–8. [PubMed: 18045124]
- 124.
- Olivius C, Landin-Wilhelmsen K, Olsson DS, Johannsson G, Tivesten Å. Prevalence and treatment of central hypogonadism and hypoandrogenism in women with hypopituitarism. Pituitary. 2018;21(5):445–53. [PubMed: 29789996]
- 125.
- Sanmartí A, Lucas A, Hawkins F, Webb SM, Ulied A. Observational study in adult hypopituitary patients with untreated growth hormone deficiency (ODA study). Socio-economic impact and health status. Collaborative ODA (Observational GH Deficiency in Adults) Group. Eur J Endocrinol. 1999;141(5):481–9. [PubMed: 10576764]
- 126.
- Clemmons DR. Consensus statement on the standardization and evaluation of growth hormone and insulin-like growth factor assays. ClinChem. 2011;57(4):555–9. [PubMed: 21285256]
- 127.
- Garcia JM, Biller BMK, Korbonits M, Popovic V, Luger A, Strasburger CJ, et al. Sensitivity and specificity of the macimorelin test for diagnosis of AGHD. Endocrine connections. 2021;10(1):76–83. [PMC free article: PMC7923131] [PubMed: 33320108]
- 128.
- Roth J, Glick SM, Yalow RS. Bersonsa. Hypoglycemia: a potent stimulus to secretion of growth hormone. Science (New York, NY). 1963;140(3570):987–8. [PubMed: 13975313]
- 129.
- Hoffman DM, O'Sullivan AJ, Baxter RC, Ho KK. Diagnosis of growth-hormone deficiency in adults. Lancet. 1994;343(8905):1064–8. [PubMed: 7512681]
- 130.
- Hoeck HC, Vestergaard P, Jakobsen PE, Laurberg P. Test of growth hormone secretion in adults: poor reproducibility of the insulin tolerance test. Eur J Endocrinol. 1995;133(3):305–12. [PubMed: 7581946]
- 131.
- Fisker S, Jorgensen JO, Orskov H, Christiansen JS. L-arginine and insulin-tolerance tests in the diagnosis of adult growth hormone deficiency: influence of confounding factors. Clinical Endocrinology. 1998;48(1):109–15. [PubMed: 9509076]
- 132.
- Shah A, Stanhope R, Matthew D. Hazards of pharmacological tests of growth hormone secretion in childhood. Bmj. 1992;304(6820):173–4. [PMC free article: PMC1881200] [PubMed: 1737165]
- 133.
- Lange M, Svendsen OL, Skakkebaek NE, Muller J, Juul A, Schmiegelow M, et al. An audit of the insulin-tolerance test in 255 patients with pituitary disease. European Journal of Endocrinology. 2002;147(1):41–7. [PubMed: 12088918]
- 134.
- Andersen M. The robustness of diagnostic tests for GH deficiency in adults. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2015;25(3):108-14. [PubMed: 25900364]
- 135.
- Corneli G, Di Somma C, Baldelli R, Rovere S, Gasco V, Croce CG, et al. The cut-off limits of the GH response to GH-releasing hormone-arginine test related to body mass index. European Journal of Endocrinology. 2005;153(2):257–64. [PubMed: 16061832]
- 136.
- Aimaretti G, Corneli G, Razzore P, Bellone S, Baffoni C, Arvat E, et al. Comparison between insulin-induced hypoglycemia and growth hormone (GH)-releasing hormone + arginine as provocative tests for the diagnosis of GH deficiency in adults. The Journal of Clinical Endocrinology and Metabolism. 1998;83(5):1615–8. [PubMed: 9589665]
- 137.
- Abs R. Update on the diagnosis of GH deficiency in adults. Eur J Endocrinol. 2003;148 Suppl 2:S3–8. [PubMed: 12670294]
- 138.
- Yuen KC, Biller BM, Molitch ME, Cook DM. Clinical review: Is lack of recombinant growth hormone (GH)-releasing hormone in the United States a setback or time to consider glucagon testing for adult GH deficiency? J Clin Endocrinol Metab. 2009;94(8):2702–7. [PubMed: 19509104]
- 139.
- Diri H, Karaca Z, Simsek Y, Tanriverdi F, Unluhizarci K, Selcuklu A, et al. Can a glucagon stimulation test characterized by lower GH cut-off value be used for the diagnosis of growth hormone deficiency in adults? Pituitary. 2015;18(6):884–92. [PubMed: 26129876]
- 140.
- Hamrahian AH, Yuen KC, Gordon MB, Pulaski-Liebert KJ, Bena J, Biller BM. Revised GH and cortisol cut-points for the glucagon stimulation test in the evaluation of GH and hypothalamic-pituitary-adrenal axes in adults: results from a prospective randomized multicenter study. Pituitary. 2016;19(3):332–41. [PubMed: 26897383]
- 141.
- Tavares AB, Seixas-da-Silva IA, Silvestre DH, Paixão CM, Jr., Vaisman M, Conceição FL. Potential risks of glucagon stimulation test in elderly people. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2015;25(1):53-6. [PubMed: 25481820]
- 142.
- Toogood AA, O'Neill PA, Shalet SM. Beyond the somatopause: growth hormone deficiency in adults over the age of 60 years. J Clin Endocrinol Metab. 1996;81(2):460–5. [PubMed: 8636250]
- 143.
- Yuen KC, Biller BM, Katznelson L, Rhoads SA, Gurel MH, Chu O, et al. Clinical characteristics, timing of peak responses and safety aspects of two dosing regimens of the glucagon stimulation test in evaluating growth hormone and cortisol secretion in adults. Pituitary. 2013;16(2):220–30. [PubMed: 22806554]
- 144.
- Micmacher E, Assumpção RP, Redorat RG, Spina LD, Cruz IC, Silva CA, et al. Growth hormone secretion in response to glucagon stimulation test in healthy middle-aged men. Arquivos brasileiros de endocrinologia e metabologia. 2009;53(7):853–8. [PubMed: 19942987]
- 145.
- Wilson JR, Utz AL, Devin JK. Effects of gender, body weight, and blood glucose dynamics on the growth hormone response to the glucagon stimulation test in patients with pituitary disease. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2016;26:24-31. [PMC free article: PMC4716555] [PubMed: 26774402]
- 146.
- Biller BM, Samuels MH, Zagar A, Cook DM, Arafah BM, Bonert V, et al. Sensitivity and specificity of six tests for the diagnosis of adult GH deficiency. The Journal of Clinical Endocrinology and Metabolism. 2002;87(5):2067–79. [PubMed: 11994342]
- 147.
- Junnila RK, Strasburger CJ, Bidlingmaier M. Pitfalls of insulin-like growth factor-i and growth hormone assays. Endocrinology and metabolism clinics of North America. 2015;44(1):27–34. [PubMed: 25732639]
- 148.
- Pokrajac A, Wark G, Ellis AR, Wear J, Wieringa GE, Trainer PJ. Variation in GH and IGF-I assays limits the applicability of international consensus criteria to local practice. Clin Endocrinol (Oxf). 2007;67(1):65–70. [PubMed: 17437512]
- 149.
- Toogood A, Brabant G, Maiter D, Jonsson B, Feldt-Rasmussen U, Koltowska-Haggstrom M, et al. Similar clinical features among patients with severe adult growth hormone deficiency diagnosed with insulin tolerance test or arginine or glucagon stimulation tests. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2012;18(3):325-34. [PubMed: 22068248]
- 150.
- Andersen M, Støving RK, Hangaard J, Petersen PH, Hagen C. The effect of short-term cortisol changes on growth hormone responses to the pyridostigmine-growth-hormone-releasing-hormone test in healthy adults and patients with suspected growth hormone deficiency. Clin Endocrinol (Oxf). 1998;49(2):241–9. [PubMed: 9828914]
- 151.
- Dichtel LE, Yuen KC, Bredella MA, Gerweck AV, Russell BM, Riccio AD, et al. Overweight/Obese adults with pituitary disorders require lower peak growth hormone cutoff values on glucagon stimulation testing to avoid overdiagnosis of growth hormone deficiency. The Journal of Clinical Endocrinology and Metabolism. 2014;99(12):4712–9. [PMC free article: PMC4255132] [PubMed: 25210883]
- 152.
- Toogood AA, Beardwell CG, Shalet SM. The severity of growth hormone deficiency in adults with pituitary disease is related to the degree of hypopituitarism. Clinical Endocrinology. 1994;41(4):511–6. [PubMed: 7955461]
- 153.
- Aimaretti G, Corneli G, Di Somma C, Baldelli R, Gasco V, Rovere S, et al. Different degrees of GH deficiency evidenced by GHRH+arginine test and IGF-I levels in adults with pituritary disease. JEndocrinolInvest. 2005;28(3):247–52. [PubMed: 15952410]
- 154.
- Gordon MB, Levy RA, Gut R, Germak J. TRENDS IN GROWTH HORMONE STIMULATION TESTING AND GROWTH HORMONE DOSING IN ADULT GROWTH HORMONE DEFICIENCY PATIENTS: RESULTS FROM THE ANSWER PROGRAM. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2016;22(4):396-405. [PubMed: 26574788]
- 155.
- Sonksen PH. In: Adashi EY, Thorner MO, editors. The somatotrophic axis and the reproductive process in health and disease. New York: Springer-Verlag; 1995. [PubMed: 8194609]
- 156.
- Schneider HJ, Kreitschmann-Andermahr I, Ghigo E, Stalla GK, Agha A. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA. 2007;298(12):1429–38. [PubMed: 17895459]
- 157.
- Garrahy A, Sherlock M, Thompson CJ. MANAGEMENT OF ENDOCRINE DISEASE: Neuroendocrine surveillance and management of neurosurgical patients. Eur J Endocrinol. 2017;176(5):R217–r33. [PubMed: 28193628]
- 158.
- Murray RD, Skillicorn CJ, Howell SJ, Lissett CA, Rahim A, Shalet SM. Dose titration and patient selection increases the efficacy of GH replacement in severely GH deficient adults. Clin Endocrinol (Oxf). 1999;50(6):749–57. [PubMed: 10468947]
- 159.
- Wirén L, Bengtsson BA, Johannsson G. Beneficial effects of long-term GH replacement therapy on quality of life in adults with GH deficiency. Clin Endocrinol (Oxf). 1998;48(5):613–20. [PubMed: 9666873]
- 160.
- Gibney J, Wallace JD, Spinks T, Schnorr L, Ranicar A, Cuneo RC, et al. The effects of 10 years of recombinant human growth hormone (GH) in adult GH-deficient patients. J Clin Endocrinol Metab. 1999;84(8):2596–602. [PubMed: 10443645]
- 161.
- Koltowska-Haggstrom M, Mattsson AF, Monson JP, Kind P, Badia X, Casanueva FF, et al. Does long-term GH replacement therapy in hypopituitary adults with GH deficiency normalise quality of life? European Journal of Endocrinology. 2006;155(1):109–19. [PubMed: 16793956]
- 162.
- Miller KK, Wexler T, Fazeli P, Gunnell L, Graham GJ, Beauregard C, et al. Growth hormone deficiency after treatment of acromegaly: a randomized, placebo-controlled study of growth hormone replacement. J Clin Endocrinol Metab. 2010;95(2):567–77. [PMC free article: PMC2840863] [PubMed: 20061426]
- 163.
- Valassi E, Brick DJ, Johnson JC, Biller BM, Klibanski A, Miller KK. Effect of growth hormone replacement therapy on the quality of life in women with growth hormone deficiency who have a history of acromegaly versus other disorders. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2012;18(2):209-18. [PMC free article: PMC3677776] [PubMed: 22440981]
- 164.
- Klose M, Rasmussen AK, Feldt-Rasmussen U. Quality of Life in adult hypopituitary patiens treated for growth hormone deficiency. The Open Endocrinology Journal. 2012;6:91–102.
- 165.
- Baum HB, Katznelson L, Sherman JC, Biller BM, Hayden DL, Schoenfeld DA, et al. Effects of physiological growth hormone (GH) therapy on cognition and quality of life in patients with adult-onset GH deficiency. The Journal of Clinical Endocrinology and Metabolism. 1998;83(9):3184–9. [PubMed: 9745423]
- 166.
- Nyberg F, Burman P. Growth hormone and its receptors in the central nervous system--location and functional significance. Hormone research. 1996;45(1-2):18–22. [PubMed: 8742113]
- 167.
- Burman P, Hetta J, Wide L, Mansson JE, Ekman R, Karlsson FA. Growth hormone treatment affects brain neurotransmitters and thyroxine. Clinical Endocrinology. 1996;44(3):319–24. [see comment] [PubMed: 8729530]
- 168.
- Nyberg F. Aging effects on growth hormone receptor binding in the brain. Experimental gerontology. 1997;32(4-5):521–8. [PubMed: 9315453]
- 169.
- Lai Z, Roos P, Zhai O, Olsson Y, Fhölenhag K, Larsson C, et al. Age-related reduction of human growth hormone-binding sites in the human brain. Brain research. 1993;621(2):260–6. [PubMed: 8242339]
- 170.
- Chikani V, Cuneo RC, Hickman I, Ho KK. Growth hormone (GH) enhances anaerobic capacity: impact on physical function and quality of life in adults with GH deficiency. Clin Endocrinol (Oxf). 2016;85(4):660–8. [PubMed: 27346880]
- 171.
- Hull KL, Harvey S. Growth hormone therapy and Quality of Life: possibilities, pitfalls and mechanisms. The Journal of endocrinology. 2003;179(3):311–33. [PubMed: 14656202]
- 172.
- Hazem A, Elamin MB, Bancos I, Malaga G, Prutsky G, Domecq JP, et al. Body composition and quality of life in adults treated with GH therapy: a systematic review and meta-analysis. Eur J Endocrinol. 2012;166(1):13–20. [PubMed: 21865409]
- 173.
- Drake WM, Coyte D, Camacho-Hübner C, Jivanji NM, Kaltsas G, Wood DF, et al. Optimizing growth hormone replacement therapy by dose titration in hypopituitary adults. J Clin Endocrinol Metab. 1998;83(11):3913–9. [PubMed: 9814468]
- 174.
- Jørgensen JO, Pedersen SA, Laurberg P, Weeke J, Skakkebaek NE, Christiansen JS. Effects of growth hormone therapy on thyroid function of growth hormone-deficient adults with and without concomitant thyroxine-substituted central hypothyroidism. J Clin Endocrinol Metab. 1989;69(6):1127–32. [PubMed: 2685007]
- 175.
- Florakis D, Hung V, Kaltsas G, Coyte D, Jenkins PJ, Chew SL, et al. Sustained reduction in circulating cholesterol in adult hypopituitary patients given low dose titrated growth hormone replacement therapy: a two year study. Clin Endocrinol (Oxf). 2000;53(4):453–9. [PubMed: 11012570]
- 176.
- Abrahamsen B, Nielsen TL, Hangaard J, Gregersen G, Vahl N, Korsholm L, et al. Dose-, IGF-I- and sex-dependent changes in lipid profile and body composition during GH replacement therapy in adult onset GH deficiency. Eur J Endocrinol. 2004;150(5):671–9. [PubMed: 15132723]
- 177.
- Lind S, Rudling M, Ericsson S, Olivecrona H, Eriksson M, Borgström B, et al. Growth hormone induces low-density lipoprotein clearance but not bile acid synthesis in humans. Arteriosclerosis, thrombosis, and vascular biology. 2004;24(2):349–56. [PubMed: 14656733]
- 178.
- Attanasio AF, Bates PC, Ho KK, Webb SM, Ross RJ, Strasburger CJ, et al. Human growth hormone replacement in adult hypopituitary patients: long-term effects on body composition and lipid status--3-year results from the HypoCCS Database. J Clin Endocrinol Metab. 2002;87(4):1600–6. [PubMed: 11932289]
- 179.
- Höybye C, Christiansen JS. Growth hormone replacement in adults - current standards and new perspectives. Best practice & research Clinical endocrinology & metabolism. 2015;29(1):115–23. [PubMed: 25617177]
- 180.
- van Bunderen CC, van den Dries CJ, Heymans MW, Franken AA, Koppeschaar HP, van der Lely AJ, et al. Effect of long-term GH replacement therapy on cardiovascular outcomes in isolated GH deficiency compared with multiple pituitary hormone deficiencies: a sub-analysis from the Dutch National Registry of Growth Hormone Treatment in Adults. Eur J Endocrinol. 2014;171(2):151–60. [PubMed: 24801587]
- 181.
- Kreitschmann-Andermahr I, Siegel S, Francis F, Buchfelder M, Schneider HJ, Kann PH, et al. Variation of the baseline characteristics and treatment parameters over time: an analysis of 15 years of growth hormone replacement in adults in the German KIMS database. Pituitary. 2012;15 Suppl 1:S72–80. [PubMed: 22829164]
- 182.
- Abrams P, Boquete H, Fideleff H, Feldt-Rasmussen U, Jönsson PJ, Koltowska-Häggström M, et al. GH replacement in hypopituitarism improves lipid profile and quality of life independently of changes in obesity variables. Eur J Endocrinol. 2008;159(6):825–32. [PubMed: 18713841]
- 183.
- Olivecrona H, Ericsson S, Berglund L, Angelin B. Increased concentrations of serum lipoprotein (a) in response to growth hormone treatment. Bmj. 1993;306(6894):1726–7. [PMC free article: PMC1678311] [PubMed: 8343630]
- 184.
- Svensson J, Jansson JO, Ottosson M, Johannsson G, Taskinen MR, Wiklund O, et al. Treatment of obese subjects with the oral growth hormone secretagogue MK-677 affects serum concentrations of several lipoproteins, but not lipoprotein(a). J Clin Endocrinol Metab. 1999;84(6):2028–33. [PubMed: 10372705]
- 185.
- Wieringa G, Toogood AA, Ryder WD, Anderson JM, Mackness M, Shalet SM. Changes in lipoprotein(a) levels measured by six kit methods during growth hormone treatment of growth hormone-deficient adults. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2000;10(1):14-9. [PubMed: 10753588]
- 186.
- Weber MM, Biller BM, Pedersen BT, Pournara E, Christiansen JS, Höybye C. The effect of growth hormone (GH) replacement on blood glucose homeostasis in adult nondiabetic patients with GH deficiency: real-life data from the NordiNet(®) International Outcome Study. Clin Endocrinol (Oxf). 2017;86(2):192–8. [PubMed: 27736009]
- 187.
- Bollerslev J, Hallén J, Fougner KJ, Jørgensen AP, Kristo C, Fagertun H, et al. Low-dose GH improves exercise capacity in adults with GH deficiency: effects of a 22-month placebo-controlled, crossover trial. Eur J Endocrinol. 2005;153(3):379–87. [PubMed: 16131600]
- 188.
- Widdowson WM, Gibney J. The effect of growth hormone (GH) replacement on muscle strength in patients with GH-deficiency: a meta-analysis. Clin Endocrinol (Oxf). 2010;72(6):787–92. [PubMed: 19769614]
- 189.
- Sneppen SB, Hoeck HC, Kollerup G, Sørensen OH, Laurberg P, Feldt-Rasmussen U. Bone mineral content and bone metabolism during physiological GH treatment in GH-deficient adults--an 18-month randomised, placebo-controlled, double blinded trial. Eur J Endocrinol. 2002;146(2):187–95. [PubMed: 11834427]
- 190.
- Johannsson G, Rosén T, Bosaeus I, Sjöström L, Bengtsson BA. Two years of growth hormone (GH) treatment increases bone mineral content and density in hypopituitary patients with adult-onset GH deficiency. J Clin Endocrinol Metab. 1996;81(8):2865–73. [PubMed: 8768843]
- 191.
- Holmes SJ, Whitehouse RW, Swindell R, Economou G, Adams JE, Shalet SM. Effect of growth hormone replacement on bone mass in adults with adult onset growth hormone deficiency. Clin Endocrinol (Oxf). 1995;42(6):627–33. [PubMed: 7634504]
- 192.
- Barake M, Klibanski A, Tritos NA. Effects of recombinant human growth hormone therapy on bone mineral density in adults with growth hormone deficiency: a meta-analysis. J Clin Endocrinol Metab. 2014;99(3):852–60. [PubMed: 24423364]
- 193.
- Rahim A, Holmes SJ, Adams JE, Shalet SM. Long-term change in the bone mineral density of adults with adult onset growth hormone (GH) deficiency in response to short or long-term GH replacement therapy. Clin Endocrinol (Oxf). 1998;48(4):463–9. [PubMed: 9640413]
- 194.
- Davidson P, Milne R, Chase D, Cooper C. Growth hormone replacement in adults and bone mineral density: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2004;60(1):92–8. [PubMed: 14678294]
- 195.
- Clanget C, Seck T, Hinke V, Wüster C, Ziegler R, Pfeilschifter J. Effects of 6 years of growth hormone (GH) treatment on bone mineral density in GH-deficient adults. Clin Endocrinol (Oxf). 2001;55(1):93–9. [PubMed: 11453957]
- 196.
- Appelman-Dijkstra NM, Claessen KM, Hamdy NA, Pereira AM, Biermasz NR. Effects of up to 15 years of recombinant human GH (rhGH) replacement on bone metabolism in adults with growth hormone deficiency (GHD): the Leiden Cohort Study. Clin Endocrinol (Oxf). 2014;81(5):727–35. [PubMed: 24816144]
- 197.
- Tritos NA, Hamrahian AH, King D, Greenspan SL, Cook DM, Jönsson PJ, et al. Predictors of the effects of 4 years of growth hormone replacement on bone mineral density in patients with adult-onset growth hormone deficiency - a KIMS database analysis. Clin Endocrinol (Oxf). 2013;79(2):178–84. [PMC free article: PMC4891937] [PubMed: 23278636]
- 198.
- Holmer H, Svensson J, Rylander L, Johannsson G, Rosén T, Bengtsson BA, et al. Fracture incidence in GH-deficient patients on complete hormone replacement including GH. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2007;22(12):1842-50. [PubMed: 17725379]
- 199.
- Mo D, Fleseriu M, Qi R, Jia N, Child CJ, Bouillon R, et al. Fracture risk in adult patients treated with growth hormone replacement therapy for growth hormone deficiency: a prospective observational cohort study. The lancet Diabetes & endocrinology. 2015;3(5):331–8. [PubMed: 25876453]
- 200.
- Klefter O, Feldt-Rasmussen U. Is increase in bone mineral content caused by increase in skeletal muscle mass/strength in adult patients with GH-treated GH deficiency? A systematic literature analysis. Eur J Endocrinol. 2009;161(2):213–21. [PubMed: 19439507]
- 201.
- Monson JP, Abs R, Bengtsson BA, Bennmarker H, Feldt-Rasmussen U, Hernberg-Stâhl E, et al. Growth hormone deficiency and replacement in elderly hypopituitary adults. KIMS Study Group and the KIMS International Board. Pharmacia and Upjohn International Metabolic Database. Clin Endocrinol (Oxf). 2000;53(3):281–9. [PubMed: 10971444]
- 202.
- Fernholm R, Bramnert M, Hägg E, Hilding A, Baylink DJ, Mohan S, et al. Growth hormone replacement therapy improves body composition and increases bone metabolism in elderly patients with pituitary disease. J Clin Endocrinol Metab. 2000;85(11):4104–12. [PubMed: 11095440]
- 203.
- Kokshoorn NE, Biermasz NR, Roelfsema F, Smit JW, Pereira AM, Romijn JA. GH replacement therapy in elderly GH-deficient patients: a systematic review. Eur J Endocrinol. 2011;164(5):657–65. [PubMed: 21339335]
- 204.
- Vahl N, Juul A, Jørgensen JO, Orskov H, Skakkebaek NE, Christiansen JS. Continuation of growth hormone (GH) replacement in GH-deficient patients during transition from childhood to adulthood: a two-year placebo-controlled study. J Clin Endocrinol Metab. 2000;85(5):1874–81. [PubMed: 10843168]
- 205.
- Carroll PV, Drake WM, Maher KT, Metcalfe K, Shaw NJ, Dunger DB, et al. Comparison of continuation or cessation of growth hormone (GH) therapy on body composition and metabolic status in adolescents with severe GH deficiency at completion of linear growth. J Clin Endocrinol Metab. 2004;89(8):3890–5. [PubMed: 15292323]
- 206.
- Drake WM, Carroll PV, Maher KT, Metcalfe KA, Camacho-Hübner C, Shaw NJ, et al. The effect of cessation of growth hormone (GH) therapy on bone mineral accretion in GH-deficient adolescents at the completion of linear growth. J Clin Endocrinol Metab. 2003;88(4):1658–63. [PubMed: 12679453]
- 207.
- Courtillot C, Baudoin R, Du Souich T, Saatdjian L, Tejedor I, Pinto G, et al. Monocentric study of 112 consecutive patients with childhood onset GH deficiency around and after transition. Eur J Endocrinol. 2013;169(5):587–96. [PubMed: 23939920]
- 208.
- Clayton PE, Cuneo RC, Juul A, Monson JP, Shalet SM, Tauber M. Consensus statement on the management of the GH-treated adolescent in the transition to adult care. Eur J Endocrinol. 2005;152(2):165–70. [PubMed: 15745921]
- 209.
- Toogood AA, Taylor NF, Shalet SM, Monson JP. Modulation of cortisol metabolism by low-dose growth hormone replacement in elderly hypopituitary patients. J Clin Endocrinol Metab. 2000;85(4):1727–30. [PubMed: 10770221]
- 210.
- Agha A, Walker D, Perry L, Drake WM, Chew SL, Jenkins PJ, et al. Unmasking of central hypothyroidism following growth hormone replacement in adult hypopituitary patients. Clin Endocrinol (Oxf). 2007;66(1):72–7. [PubMed: 17201804]
- 211.
- Jørgensen JO, Møller J, Laursen T, Orskov H, Christiansen JS, Weeke J. Growth hormone administration stimulates energy expenditure and extrathyroidal conversion of thyroxine to triiodothyronine in a dose-dependent manner and suppresses circadian thyrotrophin levels: studies in GH-deficient adults. Clin Endocrinol (Oxf). 1994;41(5):609–14. [PubMed: 7828350]
- 212.
- Jørgensen JO, Møller J, Skakkebaek NE, Weeke J, Christiansen JS. Thyroid function during growth hormone therapy. Hormone research. 1992;38 Suppl 1:63–7. [PubMed: 1295815]
- 213.
- Laurberg P, Jakobsen PE, Hoeck HC, Vestergaard P. Growth hormone and thyroid function: is secondary thyroid failure underdiagnosed in growth hormone deficient patients? Thyroidology. 1994;6(3):73–9. [PubMed: 7544998]
- 214.
- Span JP, Pieters GF, Sweep CG, Hermus AR, Smals AG. Gender difference in insulin-like growth factor I response to growth hormone (GH) treatment in GH-deficient adults: role of sex hormone replacement. J Clin Endocrinol Metab. 2000;85(3):1121–5. [PubMed: 10720049]
- 215.
- Wolthers T, Hoffman DM, Nugent AG, Duncan MW, Umpleby M, Ho KK. Oral estrogen antagonizes the metabolic actions of growth hormone in growth hormone-deficient women. American journal of physiology Endocrinology and metabolism. 2001;281(6):E1191–6. [PubMed: 11701433]
- 216.
- Birzniece V, Ho KKY. Sex steroids and the GH axis: Implications for the management of hypopituitarism. Best practice & research Clinical endocrinology & metabolism. 2017;31(1):59–69. [PubMed: 28477733]
- 217.
- Christiansen JJ, Fisker S, Gravholt CH, Bennett P, Svenstrup B, Andersen M, et al. Discontinuation of estrogen replacement therapy in GH-treated hypopituitary women alters androgen status and IGF-I. Eur J Endocrinol. 2005;152(5):719–26. [PubMed: 15879357]
- 218.
- Weissberger AJ, Ho KK, Lazarus L. Contrasting effects of oral and transdermal routes of estrogen replacement therapy on 24-hour growth hormone (GH) secretion, insulin-like growth factor I, and GH-binding protein in postmenopausal women. The Journal of Clinical Endocrinology and Metabolism. 1991;72(2):374–81. [PubMed: 1991807]
- 219.
- Brooke AM, Kalingag LA, Miraki-Moud F, Camacho-Hübner C, Maher KT, Walker DM, et al. Dehydroepiandrosterone (DHEA) replacement reduces growth hormone (GH) dose requirement in female hypopituitary patients on GH replacement. Clin Endocrinol (Oxf). 2006;65(5):673–80. [PubMed: 17054472]
- 220.
- Arlt W, Callies F, van Vlijmen JC, Koehler I, Reincke M, Bidlingmaier M, et al. Dehydroepiandrosterone replacement in women with adrenal insufficiency. N Engl J Med. 1999;341(14):1013–20. [PubMed: 10502590]
- 221.
- van Thiel SW, Romijn JA, Pereira AM, Biermasz NR, Roelfsema F, van Hemert A, et al. Effects of dehydroepiandrostenedione, superimposed on growth hormone substitution, on quality of life and insulin-like growth factor I in patients with secondary adrenal insufficiency: a randomized, placebo-controlled, cross-over trial. J Clin Endocrinol Metab. 2005;90(6):3295–303. [PubMed: 15797966]
- 222.
- Feldt-Rasmussen U, Brabant G, Maiter D, Jonsson B, Toogood A, Koltowska-Haggstrom M, et al. Response to GH treatment in adult GH deficiency is predicted by gender, age, and IGF1 SDS but not by stimulated GH-peak. Eur J Endocrinol. 2013;168(5):733–43. [PubMed: 23416951]
- 223.
- Mah PM, Webster J, Jönsson P, Feldt-Rasmussen U, Koltowska-Häggström M, Ross RJ. Estrogen replacement in women of fertile years with hypopituitarism. J Clin Endocrinol Metab. 2005;90(11):5964–9. [PubMed: 16091478]
- 224.
- Ho KKY, Gibney J, Johannsson G, Wolthers T. Regulating of growth hormone sensitivity by sex steroids: implications for therapy. Frontiers of hormone research. 2006;35:115–28. [PubMed: 16809927]
- 225.
- Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, et al. Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(11):3888–921. [PubMed: 27736313]
- 226.
- Johannsson G, Gordon MB, Højby Rasmussen M, Håkonsson IH, Karges W, Sværke C, et al. Once-weekly Somapacitan is Effective and Well Tolerated in Adults with GH Deficiency: A Randomized Phase 3 Trial. J Clin Endocrinol Metab. 2020;105(4):e1358–76. [PMC free article: PMC7076631] [PubMed: 32022863]
- 227.
- Sävendahl L, Battelino T, Højby Rasmussen M, Brod M, Saenger P, Horikawa R., Effective GH. Replacement With Once-weekly Somapacitan vs Daily GH in Children with GHD: 3-year Results From REAL 3. J Clin Endocrinol Metab. 2022;107(5):1357–67. [PMC free article: PMC9016428] [PubMed: 34964458]
- 228.
- Maniatis AK, Casella SJ, Nadgir UM, Hofman PL, Saenger P, Chertock ED, et al. Safety and Efficacy of Lonapegsomatropin in Children with Growth Hormone Deficiency: enliGHten Trial 2-Year Results. J Clin Endocrinol Metab. 2022 [PMC free article: PMC9202697] [PubMed: 35428884]
- 229.
- Deal C, Steelman J, Vlachopapadopoulou E, Stawerska R, Silverman LA, Phillip M, et al. Efficacy and safety of weekly somatrogon vs daily somatropin in children with growth hormone deficiency: a phase 3 study. J Clin Endocrinol Metab. 2022 [PMC free article: PMC9202717] [PubMed: 35405011]
- 230.
- Du H, Wu D, Yi P, Bai X, Luo Y, Yang H, et al. Evaluation of efficacy and safety of long-acting PEGylated recombinant human growth hormone (Jintrolong) for patients with growth hormone deficiency. Journal of pediatric endocrinology & metabolism. JPEM. 2022;35(4):511–7. [PubMed: 35245011]
- 231.
- Yuen KCJ, Miller BS, Boguszewski CL, Hoffman AR. Usefulness and Potential Pitfalls of Long-Acting Growth Hormone Analogs. Frontiers in endocrinology. 2021;12:637209. [PMC free article: PMC7943875] [PubMed: 33716988]
- 232.
- Cruz-Topete D, Jorgensen JO, Christensen B, Sackmann-Sala L, Krusenstjerna-Hafstrøm T, Jara A, et al. Identification of new biomarkers of low-dose GH replacement therapy in GH-deficient patients. J Clin Endocrinol Metab. 2011;96(7):2089–97. [PMC free article: PMC3205513] [PubMed: 21543428]
- 233.
- Frajese G, Drake WM, Loureiro RA, Evanson J, Coyte D, Wood DF, et al. Hypothalamo-pituitary surveillance imaging in hypopituitary patients receiving long-term GH replacement therapy. J Clin Endocrinol Metab. 2001;86(11):5172–5. [PubMed: 11701673]
- 234.
- Chung TT, Drake WM, Evanson J, Walker D, Plowman PN, Chew SL, et al. Tumour surveillance imaging in patients with extrapituitary tumours receiving growth hormone replacement. Clin Endocrinol (Oxf). 2005;63(3):274–9. [PubMed: 16117814]
- 235.
- Robison LL, Armstrong GT, Boice JD, Chow EJ, Davies SM, Donaldson SS, et al. The Childhood Cancer Survivor Study: a National Cancer Institute-supported resource for outcome and intervention research. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2009;27(14):2308–18. [PMC free article: PMC2677920] [PubMed: 19364948]
- 236.
- Mackenzie S, Craven T, Gattamaneni HR, Swindell R, Shalet SM, Brabant G. Long-term safety of growth hormone replacement after CNS irradiation. J Clin Endocrinol Metab. 2011;96(9):2756–61. [PubMed: 21715535]
- 237.
- Popovic V, Mattsson AF, Gaillard RC, Wilton P, Koltowska-Häggström M, Ranke MB. Serum insulin-like growth factor I (IGF-I), IGF-binding proteins 2 and 3, and the risk for development of malignancies in adults with growth hormone (GH) deficiency treated with GH: data from KIMS (Pfizer International Metabolic Database). J Clin Endocrinol Metab. 2010;95(9):4449–54. [PubMed: 20610598]
- 238.
- van Bunderen CC, van Nieuwpoort IC, Arwert LI, Heymans MW, Franken AA, Koppeschaar HP, et al. Does growth hormone replacement therapy reduce mortality in adults with growth hormone deficiency? Data from the Dutch National Registry of Growth Hormone Treatment in adults. J Clin Endocrinol Metab. 2011;96(10):3151–9. [PubMed: 21849531]
- 239.
- Berglund A, Gravholt CH, Olsen MS, Christiansen JS, Stochholm K. Growth hormone replacement does not increase mortality in patients with childhood-onset growth hormone deficiency. Clin Endocrinol (Oxf). 2015;83(5):677–83. [PubMed: 26147754]
- 240.
- Stochholm K, Gravholt CH, Laursen T, Laurberg P, Andersen M, Kristensen L, et al. Mortality and GH deficiency: a nationwide study. Eur J Endocrinol. 2007;157(1):9–18. [PubMed: 17609396]
- 241.
- Stochholm K, Juul S, Christiansen JS, Gravholt CH. Mortality and socioeconomic status in adults with childhood onset GH deficiency (GHD) is highly dependent on the primary cause of GHD. Eur J Endocrinol. 2012;167(5):663–70. [PubMed: 22918302]
- 242.
- Burman P, Mattsson AF, Johannsson G, Höybye C, Holmer H, Dahlqvist P, et al. Deaths among adult patients with hypopituitarism: hypocortisolism during acute stress, and de novo malignant brain tumors contribute to an increased mortality. J Clin Endocrinol Metab. 2013;98(4):1466–75. [PubMed: 23457412]
- 243.
- Erfurth EM. Update in mortality in GH-treated patients. J Clin Endocrinol Metab. 2013;98(11):4219–26. [PubMed: 24030944]
- 244.
- Carel JC, Ecosse E, Landier F, Meguellati-Hakkas D, Kaguelidou F, Rey G, et al. Long-term mortality after recombinant growth hormone treatment for isolated growth hormone deficiency or childhood short stature: preliminary report of the French SAGhE study. J Clin Endocrinol Metab. 2012;97(2):416–25. [PubMed: 22238382]
- 245.
- Hernberg-Ståhl E, Luger A, Abs R, Bengtsson BA, Feldt-Rasmussen U, Wilton P, et al. Healthcare consumption decreases in parallel with improvements in quality of life during GH replacement in hypopituitary adults with GH deficiency. J Clin Endocrinol Metab. 2001;86(11):5277–81. [PubMed: 11701692]
- 246.
- Martel-Duguech LM, Jorgensen JOL, Korbonits M, Johannsson G, Webb SM, Amadidou F, et al. ESE audit on management of Adult Growth Hormone Deficiency in clinical practice. Eur J Endocrinol. 2020 [PubMed: 33320830]
- 247.
- Yuen KCJ. Adult growth hormone deficiency guidelines: more difficult than it seems to incorporate into clinical practice universally. Eur J Endocrinol. 2021;184(4):C5–c7. [PubMed: 33524002]
- 248.
- Mancini A, Bruno C, Vergani E, Brunetti A, Palmisano G, Pontecorvi A. "Non-Classical" Indication for Provocative Testing of Growth Hormone: A Retrospective Cohort Study in Adult Patients Under Replacement Therapy. Endocrine, metabolic & immune disorders drug targets. 2021;21(8):1406–12. [PubMed: 32990548]
- ABSTRACT
- INTRODUCTION
- PREVALENCE, INCIDENCE, AND ETIOLOGY OF GH DEFICIENCY IN ADULTS
- CLINICAL FEATURES OF GH DEFICIENCY IN ADULTS
- DIAGNOSTIC PROCEDURES
- RESPONSE TO GH REPLACEMENT IN ADULT GROWTH HORMONE DEFICIENCY
- GH REPLACEMENT IN ELDERLY HYPOPITUITARY PATIENTS
- TRANSITION BETWEEN PEDIATRIC AND ADULT CARE FOR CHILDHOOD ONSET GH DEFICIENCY
- INTERACTIONS WITH OTHER PITUITARY AND ADRENAL HORMONES
- GROWTH HORMONE REPLACEMENT
- COSTS VERSUS BENEFITS OF GH REPLACEMENT THERAPY
- ADHERENCE TO MANAGEMENT OF ADULT GROWTH HORMONE DEFICIENCY IN CLINICAL PRACTICE
- REFERENCES
- Adult Growth Hormone Deficiency- Clinical Management - EndotextAdult Growth Hormone Deficiency- Clinical Management - Endotext
- insulin-induced gene 2 protein isoform 2 [Mus musculus]insulin-induced gene 2 protein isoform 2 [Mus musculus]gi|2756223990|ref|NP_001418221.1|Protein
Your browsing activity is empty.
Activity recording is turned off.
See more...