Introduction
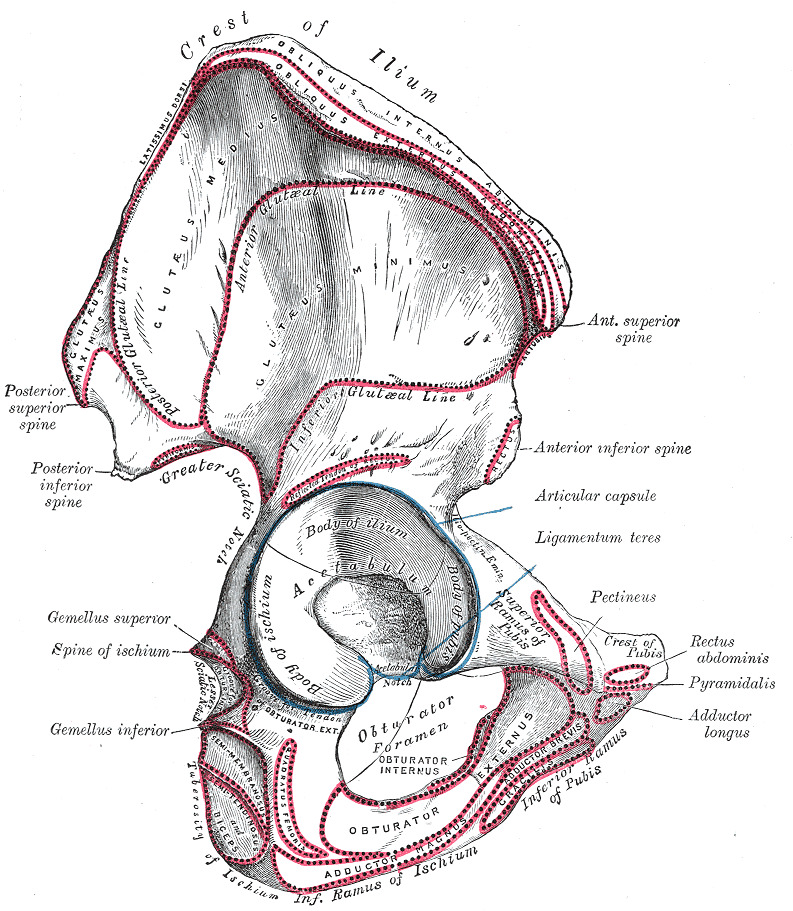
Anterior inferior iliac spine (AIIS) injuries are a distinctive and clinically significant subset of pelvic injuries. The AIIS is a bony prominence at the ilium's anterior border and superior acetabular margin (see Image. Hip Anatomy). This structure serves as an attachment point for the iliacus muscle and the origin of the rectus femoris' straight head. AIIS injuries can arise from trauma or repetitive stress, making them particularly relevant in sports medicine and orthopedic practices.[1]
The injury mechanism often involves forceful hip flexion, as seen in activities such as kicking, sprinting, or sudden direction changes, particularly in adolescents. Avulsion fractures arise when the attached muscles pull a fragment of the AIIS away from the bone or as overuse syndromes involving inflammation and microtrauma. In adolescents and young adults, the AIIS is near the growth plate. Thus, damage to this area in growing individuals can affect bone growth and development.[2] Besides isolated injuries, the AIIS has been implicated in various hip pathologies, including femoroacetabular impingement (FAI). Clinicians increasingly recognize the need for a comprehensive understanding of the anatomical, biomechanical, and clinical aspects of AIIS injuries.
Etiology
AIIS avulsion fractures typically result from a sudden, forceful rectus femoris contraction, commonly experienced by athletes engaging in activities requiring explosive lower-limb movements. Muscle pull on the developing pelvis produces this injury, posing a heightened risk to adolescents with still-maturing growth plates.[3] The rectus femoris, a quadriceps component originating from the AIIS and extending to the extensor mechanism distally, is integral in activities involving rapid hip flexion and knee extension, like kicking or sprinting, where its activation can exert excessive AIIS tension and potentially fracture the bone.
Epidemiology
AIIS avulsion is relatively rare. However, the condition exhibits specific epidemiological trends. These fractures predominantly affect adolescents and young adults, with a peak incidence during the adolescent growth spurt. The vulnerability is attributed to the open growth plates in this age group. Using the Risser classification to grade skeletal maturity, older patients are more likely to sustain iliac apophysis (anterior superior iliac spine and iliac crest) injuries. In contrast, younger patients are more likely to develop AIIS or ischial tuberosity injuries. Complete pelvic apophyseal ossification timing accounts for these differences, with the AIIS secondary ossification center closing first and the iliac apophyses closing last.[4]
Identifying risk factors, such as previous injuries or muscle imbalances, can aid in preventive strategies. Sports-related activities, particularly those involving forceful lower limb movements such as soccer, football, and track and field, account for a significant proportion of AIIS avulsion fractures.[5] Boys are more commonly affected than girls due to muscle mass and strength differences. The incidence also varies based on cultural factors, with certain sports being more popular and predisposing individuals to this injury in specific geographic regions. Seasonal variation influences the condition's incidence, with certain sports being more frequently played during particular times of the year.[6]
Pathophysiology
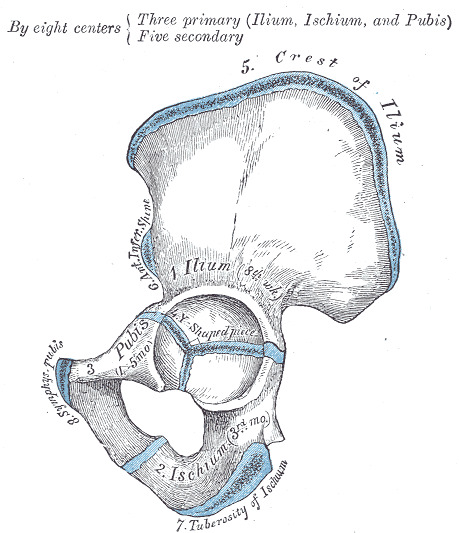
AIIS avulsion's underlying mechanism involves the rectus femoris' biomechanics during powerful eccentric contractions, illustrating the intricate interplay between physical activity, anatomical structure, and physiological development.[7] Essentially a traction phenomenon, this injury mechanism produces conditions ranging from minor avulsions to complete fractures. The mechanism is triggered by activities necessitating sudden hip flexion and knee extension, such as kicking or sprinting. Adolescents with open growth plates face heightened risk due to the pelvis' developmental state, particularly vulnerable at the tendon-bone interface where the yet-to-ossify apophysis is prone to separation under stress (see Image. Hip Bone Development).[8]
Additionally, reduced trabecular bone density in the anterior and posterior pelvic rims, as noted by Cunningham and Black, renders these areas more susceptible to injury. Growth plates are also relatively more delicate than musculotendinous units, which experience a hormonal surge in strength during growth spurts. Thus, intense muscle contractions can easily fracture developing pelvic areas by avulsion.[9]
History and Physical
A comprehensive history should identify injury mechanism details, predisposing factors, and previous hip or pelvic trauma or overuse injuries. Patients with AIIS injuries typically present with acute groin or anterior hip pain following an activity involving forceful hip flexion combined with knee extension, such as kicking, sprinting, or rapid acceleration-deceleration movements. The pain is sharp and localized to the anterior pelvic region, exacerbated by hip flexion when walking, running, or stair-climbing. Patients may report an inability to bear weight on the affected limb. Inquiries about the patient's physical activity level, sports participation, and recent changes in training routines can provide insights into potential contributing factors.
On physical examination, palpation often reveals point tenderness at the AIIS. Range of motion testing may demonstrate limited and painful hip flexion. Additional signs, such as groin or anterior hip swelling and bruising, may be present, suggesting a traumatic injury. Clinicians should perform a complete musculoskeletal and neurological examination to identify any associated injuries or deficits.[10]
Evaluation
AIIS avulsion evaluation typically involves a stepwise approach aided by imaging studies. An anteroposterior pelvis x-ray is often the initial step, followed by an oblique pelvis view if needed to enhance the detection of subtle injuries. Magnetic resonance imaging (MRI) may be used to accurately assess suspected avulsion injuries and any associated soft tissue damage. MRI is particularly helpful in cases where x-ray results are inconclusive, as in many skeletally immature patients. In rare cases, computed tomography (CT) scans may be used to further evaluate bony anatomy and avulsed fragment size and displacement.[11]
Treatment / Management
Treatment selection is often based on fracture severity, displacement, and patient characteristics. No national or international guidelines specifically address AIIS avulsion management, but general apophyseal avulsion fracture treatment principles may be applied to AIIS injuries. The American Academy of Orthopaedic Surgeons and the British Orthopaedic Association recommend nonoperative management for minimally displaced fractures, with surgical intervention reserved for injuries with significant displacement.[12]
Nonoperative ManagementNonoperative management is frequently the initial approach for AIIS avulsion injuries, especially in younger individuals with open growth plates.[13][14] This strategy emphasizes rest, activity modification, and physical therapy as its core components. The 1985 Metzmaker and Pappas protocol established a 5-stage rehabilitation program applicable to all pelvic and hip apophyseal fractures.[15] While this framework provides a general timeline, contemporary protocols emphasize individualized approaches specifically tailored to AIIS injuries.[16] These protocols involve the following:
- Stage 1 (0-7 days): Ice application, analgesics, and protected weight-bearing with crutches
- Stage 2 (7-14 days but may extend to 20 days): Gentle active and passive range-of-motion exercises with continued weight-bearing assistance
- Stage 3 (4-20 days, but may extend to 30 days): Progression to resistance exercises once 75% movement is regained, gradually increasing weight-bearing
- Stage 4 (30-60 days): Focus on stretching and strengthening exercises specific to the patient's sport
- Stage 5 (after 8 weeks): Potential return to sports participation, contingent on pain-free movement and appropriate functional recovery
Operative Management
Surgical intervention may be warranted when nonoperative methods fall short or significant displacement occurs. Rajaesekhar et al suggest surgery for cases with a large fragment displacement (>2 cm) or bony exostosis formation following the original injury.[17] McKinney et al proposed a hip-and-pelvic apophyseal fracture classification system based on displacement (see Table. Classification of Hip and Pelvic Apophyseal Fractures).[18] Type 3 and type 4 injuries warrant surgery.
Table
Table. Classification of Hip and Pelvic Apophyseal Fractures.
Surgical intervention typically involves reattaching the avulsed fragment to the AIIS. Open reduction internal fixation with cortical, cannulated, or resorbable screws are all well-documented surgical techniques for AIIS avulsion fractures.[19][20][21] Arthroscopic methods may also be employed in select cases. Ultimately, the choice of surgical approach hinges on the specific fracture characteristics and the surgeon's expertise. Deciding between operative and nonoperative AIIS avulsion management requires careful consideration of the individual's age, activity level, fracture characteristics, and initial treatment response.
Differential Diagnosis
Differentiating between AIIS avulsion injuries and other conditions presenting with anterior hip or groin pain is crucial for appropriate management. This table contains common conditions presenting similarly to AIIS avulsion and their distinguishing features:
Table
Condition Signs and Symptoms
Prognosis
The prognosis for AIIS avulsion injuries is generally favorable with prompt and appropriate management, often involving conservative treatments such as rest, activity modification, and physical therapy.[22] These injuries of the growing apophysis typically heal well. However, surgery may be considered for cases with significant displacement or failed conservative measures. Recent surgical advancements, particularly minimally invasive techniques like arthroscopy, have greatly improved AIIS injury outcomes by focusing on reattaching avulsed fragments, restoring normal anatomy, and enhancing hip flexor muscle strength and flexibility. These modalities' benefits include smaller incisions, reduced infection risks, and faster recovery.[23]
Months following surgery, patients usually experience substantial pain relief, functional recovery, and a return to preinjury activities, including sports. However, surgical procedures entail risks such as heterotopic ossification, potentially causing stiffness and pain, which may be managed with NSAIDs or radiation therapy as preventive measures. Another risk is lateral femoral cutaneous nerve damage during a direct anterior approach to the hip, necessitating careful nerve localization and protection during surgery to avoid thigh sensory disturbances.[24]
Complications
Complications from AIIS avulsion injuries are relatively rare. However, pain or discomfort may continue to be triggered during activities requiring hip flexion, affecting the patient's quality of life. Neglected injuries may result in nonunion or hypertrophic nonunion. Nonunion occurs when bone ends fail to fuse. Hypertrophic nonunion entails excessive bone growth without achieving union.[25] Identifying bony bridges across the epiphyses is crucial, as these structures can impede growth through the ossification center.[26]
Significant fragment displacement may lead to nonunion if a fibrous bridge fails to form, resulting in persistent pain and functional limitations.[27] Excessive callus formation and heterotopic ossification pose additional serious complications, causing pain and restricted range of motion. Prevention involves avoiding excessive strain on the healing growth plate, including repetitive hip extension and knee flexion, until callus formation bridges the gap. Subsequently, the gradual introduction of forces can enhance strength without promoting excessive callus formation.[28]
Malunion is another potential complication that can change the hip joint's biomechanics, potentially leading to residual weakness or muscle imbalances.[29][30] A more specialized treatment approach may be required if AIIS avulsion cooccurs with other conditions impacting the pelvis or hip joint, such as labral tears or FAI.[31]
Postoperative and Rehabilitation Care
Rehabilitation is a critical component of the recovery process following an AIIS avulsion. The rehabilitation protocol should be individualized based on factors such as injury severity, treatment received, and overall patient health. Essential aspects of a typical rehabilitation protocol are listed below:
- Early mobilization: Rehabilitation typically begins with gentle range-of-motion exercises to prevent stiffness and improve joint mobility. These exercises should focus on hip flexion, extension, abduction, and rotation.
- Strengthening exercises: Progressive strengthening exercises target the muscles around the hip joint, including the quadriceps, hamstrings, adductors, and gluteal muscles. These exercises help rebuild muscle strength lost after the injury and enhance overall hip stability.
- Core strengthening: Given the importance of core stability in hip function, rehabilitation often includes exercises to strengthen the abdominal and lower back muscles. Core stability contributes to proper biomechanics during hip movements.
- Weight-bearing activities: Gradually introducing weight-bearing activities is essential for functional recovery, with exercises such as walking, jogging, and running incorporated based on individual tolerance levels.
- Balance and proprioception training: Specific exercises that challenge balance and proprioception help improve joint awareness and stability. These aspects are crucial for athletes returning to sports that involve dynamic movements.
- Functional movement patterns: Rehabilitation should include activities replicating functional movements required in daily life or sports. The program may include sport-specific drills to ensure the individual can safely return to preinjury activities.
- Pain management: Modalities such as ice, heat, or other pain-relieving techniques may be used to manage residual pain or discomfort during rehabilitation.
- Patient education: Patients should be educated throughout rehabilitation about their injury, the importance of treatment adherence, and reinjury prevention strategies.
- Gradual return to activity: Return-to-play criteria are established in collaboration with the treating physician and rehabilitation team. The progression back to full activity is carefully monitored to minimize reinjury risk.
- Long-term maintenance: Even after completing the formal rehabilitation program, individuals may be advised to continue specific exercises and maintenance activities to support long-term joint health and prevent recurrence.
Close collaboration between the patient, physical therapist, and healthcare team is crucial to ensuring a comprehensive and successful rehabilitation journey following AIIS avulsion. Regular monitoring, progress-based protocol adjustments, and open communication contribute to optimal outcomes in the recovery process.
Consultations
Practitioners in the following fields must be consulted to optimize outcomes for patients with AIIS avulsion:
- Orthopedics
- Physical therapy and rehabilitation
- Sports medicine
- Radiology
- Emergency medicine
By working together, these professionals can address various aspects of the injury, such as pain management, rehabilitation, surgical intervention, and reinjury prevention. Interprofessional collaboration enhances communication, promotes shared decision-making, and ultimately results in better patient outcomes and overall satisfaction with care.
Deterrence and Patient Education
Deterrence and patient education are crucial in managing AIIS avulsion risk, particularly among athletes and individuals engaged in high-impact or repetitive hip-flexion activities. Effective prevention strategies and informed decision-making can significantly reduce the incidence of these injuries, thus safeguarding an individual's health and athletic career. Deterrence strategies include the following:
- Strength and flexibility training: Strengthening the muscles around the hip and improving flexibility can reduce stress on the AIIS. Exercises that boost core stability, hip flexor muscles, and hamstring flexibility are especially beneficial.
- Proper technique: Ensuring correct form and technique in sports and physical activities can help minimize excessive forces on the hip joint. Coaches and trainers need to stress technique, particularly in actions like sprinting, jumping, or kicking.
- Gradual increase in activity: Avoiding sudden activity level increases can prevent overuse injuries. Gradually ramping up training intensity and duration allows the body to adjust safely.
- Preparticipation physical evaluations: Preseason evaluations can identify individuals at higher risk of AIIS avulsion injuries. These assessments should include a physical examination focused on hip strength and flexibility.
Patient education should cover the following areas:
- Understanding the risks: Educating patients, especially young athletes and their parents, about the risks associated with AIIS avulsion injuries is essential. The potential for long-term complications of improperly managed injuries should be explained.
- Recognizing symptoms: Patients must be informed about AIIS avulsion's symptoms, such as immediate groin or anterior hip pain, trouble walking, or swelling.
- Importance of rest and recovery: Highlighting the need for adequate rest and recovery following any hip injury helps patients understand the risks of returning to activities too soon, which include reinjury or chronic issues.
- Rehabilitation and return-to-play: Providing clear guidelines on rehabilitation exercises and criteria for safely returning to play can help patients manage their recovery process effectively. Realistic expectations for the recovery timeline and the importance of following a structured rehabilitation program must be emphasized.
Healthcare providers can significantly reduce the burden of AIIS avulsion injuries and enhance overall patient well-being and athletic performance by prioritizing prevention and patient education.
Pearls and Other Issues
AIIS avulsion injuries represent a significant challenge, particularly in sports medicine. The condition typically arises from sudden, forceful rectus femoris contractions commonly seen in activities like kicking, sprinting, or jumping. The AIIS, the rectus femoris and other hip flexors' attachment site, is prone to avulsion fractures when subjected to excessive tension during these movements. Diagnosis can be intricate, often necessitating a comprehensive evaluation that includes physical examination and imaging studies such as x-rays, MRI, and CT scans to assess the extent of the injury accurately.
AIIS avulsion treatment depends on various factors, including fracture severity and the patient's age and activity level. Conservative approaches, such as rest, activity modification, and physical therapy, are typically effective in many cases, facilitating satisfactory outcomes. However, surgical intervention may be warranted in cases of significant fragment displacement or failed conservative management. Recent advancements in surgical techniques, particularly minimally invasive approaches like arthroscopy, have greatly improved outcomes by focusing on reattaching the avulsed fragment and restoring normal anatomy. Despite its potential benefits, surgery carries inherent risks such as heterotopic ossification and nerve damage, emphasizing the importance of careful patient selection and surgical technique to minimize complications and promote optimal recovery.
Interprofessional care is crucial in managing complex conditions like AIIS avulsion because it ensures comprehensive evaluation and treatment. The healthcare team should address pain management, definitive treatment, rehabilitation, and reinjury avoidance to enhance patient outcomes.
Enhancing Healthcare Team Outcomes
Managing AIIS avulsion demands a multifaceted skill set from healthcare professionals for effective, patient-centered care. Essential to this process is seamless coordination and clear communication within the healthcare team to optimize patient outcomes. Emergency medicine practitioners are often the first point of contact, providing initial assessment, pain management, and patient stabilization. Radiologists assist in the diagnostic process by interpreting imaging studies, particularly x-rays, MRI, and CT scans, aiding in accurate diagnosis and treatment planning. Orthopedic surgeons and sports medicine specialists are crucial for their expertise in musculoskeletal medicine, diagnostic imaging, and surgical techniques.
Physical therapy and rehabilitation specialists collaborate closely to oversee the patient's progress and ensure adherence to the rehabilitation protocol. Advanced practitioners, including nurse practitioners and physician assistants, provide specialized care, support diagnostic efforts, and assist in developing treatment plans. Nurses are pivotal in patient education, postoperative care, and complication monitoring, whereas pharmacists focus on medication management, especially for pain control.
Effective interprofessional communication prevents misunderstandings and enhances patient care by ensuring that all team members—physicians, advanced practitioners, nurses, and other health professionals—share critical insights into the patient's progress, pain management, and rehabilitation strategies. This collective effort promotes a comprehensive understanding of the patient's condition and the creation of a unified care plan. Strategic care coordination, from diagnosis through rehabilitation, ensures continuous care that improves patient safety and team performance.
Review Questions

References
- 1.
- Reboli M, Aprato A, Vittori J, Olivero M, Bosco F, Massè A. Reevaluation of the surgical indications for anterior inferior iliac spine avulsion fractures in an acute setting - A narrative review of the current literature. J Orthop. 2023 Apr;38:20-24. [PMC free article: PMC10018387] [PubMed: 36937226]
- 2.
- Bogwasi L, Holtzhausen L, Janse van Rensburg DC, Jansen van Rensburg A, Botha T. Management of proximal rectus femoris injuries - do we know what we're doing?: A systematic review. Biol Sport. 2023 Apr;40(2):497-512. [PMC free article: PMC10108758] [PubMed: 37077795]
- 3.
- Vadhera AS, Lee JS, Sivasundaram L, Ogle M, Westrick JC, Kunze KN, Gursoy S, Chahla J. Apophyseal ilium avulsion fractures in young athletes: a systematic review and return to sport analysis. J Pediatr Orthop B. 2023 May 01;32(3):268-277. [PubMed: 36445382]
- 4.
- HOWARD FM, PIHA RJ. FRACTURES OF THE APOPHYSES IN ADOLESCENT ATHLETES. JAMA. 1965 Jun 07;192:842-4. [PubMed: 14298135]
- 5.
- Rossi F, Dragoni S. Acute avulsion fractures of the pelvis in adolescent competitive athletes: prevalence, location and sports distribution of 203 cases collected. Skeletal Radiol. 2001 Mar;30(3):127-31. [PubMed: 11357449]
- 6.
- Calderazzi F, Nosenzo A, Galavotti C, Menozzi M, Pogliacomi F, Ceccarelli F. Apophyseal avulsion fractures of the pelvis. A review. Acta Biomed. 2018 Nov 15;89(4):470-476. [PMC free article: PMC6502104] [PubMed: 30657114]
- 7.
- Sammouni O, Zari S, Najib A, Yacoubi H. Traumatic avulsion of the anterior superior and inferior iliac spines in adult: A case report. Trauma Case Rep. 2023 Aug;46:100872. [PMC free article: PMC10310933] [PubMed: 37396116]
- 8.
- Cunningham CA, Black SM. Development of the fetal ilium--challenging concepts of bipedality. J Anat. 2009 Jan;214(1):91-9. [PMC free article: PMC2667920] [PubMed: 19018881]
- 9.
- LAURENSON RD. THE PRIMARY OSSIFICATION OF THE HUMAN ILIUM. Anat Rec. 1964 Feb;148:209-17. [PubMed: 14123505]
- 10.
- Fernandez M, Wall P, O'Donnell J, Griffin D. Hip pain in young adults. Aust Fam Physician. 2014 Apr;43(4):205-9. [PubMed: 24701624]
- 11.
- Serbest S, Tosun HB, Tiftikçi U, Oktas B, Kesgin E. Anterior inferior iliac spine avulsion fracture: a series of 5 cases. Medicine (Baltimore). 2015 Feb;94(7):e562. [PMC free article: PMC4554161] [PubMed: 25700329]
- 12.
- Brock J, Punjabi S. Simultaneous Bilateral Anterior Inferior Iliac Spine Avulsion Injury in an Adolescent Cross-Country Runner. J Orthop Case Rep. 2022 Feb;12(2):5-8. [PMC free article: PMC9499151] [PubMed: 36199726]
- 13.
- Ferraro SL, Batty M, Heyworth BE, Cook DL, Miller PE, Novais EN. Acute Pelvic and Hip Apophyseal Avulsion Fractures in Adolescents: A Summary of 719 Cases. J Pediatr Orthop. 2023 Apr 01;43(4):204-210. [PubMed: 36727766]
- 14.
- Reina N, Accadbled F, de Gauzy JS. Anterior inferior iliac spine avulsion fracture: a case report in soccer playing adolescent twins. J Pediatr Orthop B. 2010 Mar;19(2):158-60. [PubMed: 19934773]
- 15.
- Metzmaker JN, Pappas AM. Avulsion fractures of the pelvis. Am J Sports Med. 1985 Sep-Oct;13(5):349-58. [PubMed: 4051093]
- 16.
- Weel H, Joosten AJP, van Bergen CJA. Apophyseal Avulsion of the Rectus Femoris Tendon Origin in Adolescent Soccer Players. Children (Basel). 2022 Jul 08;9(7) [PMC free article: PMC9320601] [PubMed: 35884000]
- 17.
- Rajasekhar C, Kumar KS, Bhamra MS. Avulsion fractures of the anterior inferior iliac spine: the case for surgical intervention. Int Orthop. 2001;24(6):364-5. [PMC free article: PMC3619920] [PubMed: 11294433]
- 18.
- McKinney BI, Nelson C, Carrion W. Apophyseal avulsion fractures of the hip and pelvis. Orthopedics. 2009 Jan;32(1):42. [PubMed: 19226032]
- 19.
- Sinikumpu JJ, Hetsroni I, Schilders E, Lempainen L, Serlo W, Orava S. Operative treatment of pelvic apophyseal avulsions in adolescent and young adult athletes: a follow-up study. Eur J Orthop Surg Traumatol. 2018 Apr;28(3):423-429. [PubMed: 29159479]
- 20.
- Maalouly J, Aouad D, Ayoubi R, Dib N, Darwish M, Saidy E, Nehme A. Anterior inferior iliac spine avulsion fracture post hip arthroscopy for Femoroacetabular impingement. Trauma Case Rep. 2020 Oct;29:100342. [PMC free article: PMC7453136] [PubMed: 32885017]
- 21.
- Pogliacomi F, Calderazzi F, Paterlini M, Ceccarelli F. Surgical treatment of anterior iliac spines fractures: our experience. Acta Biomed. 2014 Sep 24;85 Suppl 2:52-8. [PubMed: 25409719]
- 22.
- Eberbach H, Hohloch L, Feucht MJ, Konstantinidis L, Südkamp NP, Zwingmann J. Operative versus conservative treatment of apophyseal avulsion fractures of the pelvis in the adolescents: a systematical review with meta-analysis of clinical outcome and return to sports. BMC Musculoskelet Disord. 2017 Apr 19;18(1):162. [PMC free article: PMC5395880] [PubMed: 28420360]
- 23.
- Uzun M, Alpan B, Ozger H. Avulsion fractures involving the straight and reflected heads of the rectus femoris. Hip Int. 2014 Mar-Apr;24(2):206-9. [PubMed: 24500831]
- 24.
- IRVING MH. EXOSTOSIS FORMATION AFTER TRAUMATIC AVULSION OF THE ANTERIOR INFERIOR ILIAC SPINE. REPORT OF TWO CASES. J Bone Joint Surg Br. 1964 Nov;46:720-2. [PubMed: 14251456]
- 25.
- Tomaszewski KA, Popieluszko P, Henry BM, Roy J, Sanna B, Kijek MR, Walocha JA. The surgical anatomy of the lateral femoral cutaneous nerve in the inguinal region: a meta-analysis. Hernia. 2016 Oct;20(5):649-57. [PMC free article: PMC5023748] [PubMed: 27115766]
- 26.
- Jaramillo D, Hoffer FA. Cartilaginous epiphysis and growth plate: normal and abnormal MR imaging findings. AJR Am J Roentgenol. 1992 May;158(5):1105-10. [PubMed: 1566676]
- 27.
- Shibahara M, Ohnishi Y, Honda E, Matsuda DK, Uchida S. Arthroscopic Treatment of a Displaced Nonunion of the Anterior Inferior Iliac Spine Causing Extra-articular Impingement. Orthopedics. 2017 Jul 01;40(4):e725-e728. [PubMed: 28437548]
- 28.
- Burn D. Avulsion of the Anterior Inferior Iliac Spine Rehabilitation in a Rural Private Practice. Pediatr Phys Ther. 2017 Jul;29(3):E7-E11. [PubMed: 28654505]
- 29.
- Alhaneedi GA, Abdullah ASA, Ghouri SI, Abuodeh Y, Al Dosari MMAA. Avulsion fracture of anterior inferior iliac spine complicated by hypertrophic malunion causing femoroacetabular impingement: Case report. Int J Surg Case Rep. 2015;11:117-120. [PMC free article: PMC4446677] [PubMed: 25974258]
- 30.
- Schuett DJ, Bomar JD, Pennock AT. Pelvic Apophyseal Avulsion Fractures: A Retrospective Review of 228 Cases. J Pediatr Orthop. 2015 Sep;35(6):617-23. [PubMed: 25321882]
- 31.
- Hetsroni I, Poultsides L, Bedi A, Larson CM, Kelly BT. Anterior inferior iliac spine morphology correlates with hip range of motion: a classification system and dynamic model. Clin Orthop Relat Res. 2013 Aug;471(8):2497-503. [PMC free article: PMC3705064] [PubMed: 23412732]
Disclosure: Rachel Bergman declares no relevant financial relationships with ineligible companies.
Disclosure: Nicholas Greco declares no relevant financial relationships with ineligible companies.
Disclosure: Daniel Li declares no relevant financial relationships with ineligible companies.
Publication Details
Author Information and Affiliations
Authors
Rachel Bergman1; Nicholas Greco; Daniel Li2.Affiliations
Publication History
Last Update: April 20, 2024.
Copyright
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
Publisher
StatPearls Publishing, Treasure Island (FL)
NLM Citation
Bergman R, Greco N, Li D. Anterior Inferior Iliac Spine Avulsion. [Updated 2024 Apr 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.