Introduction
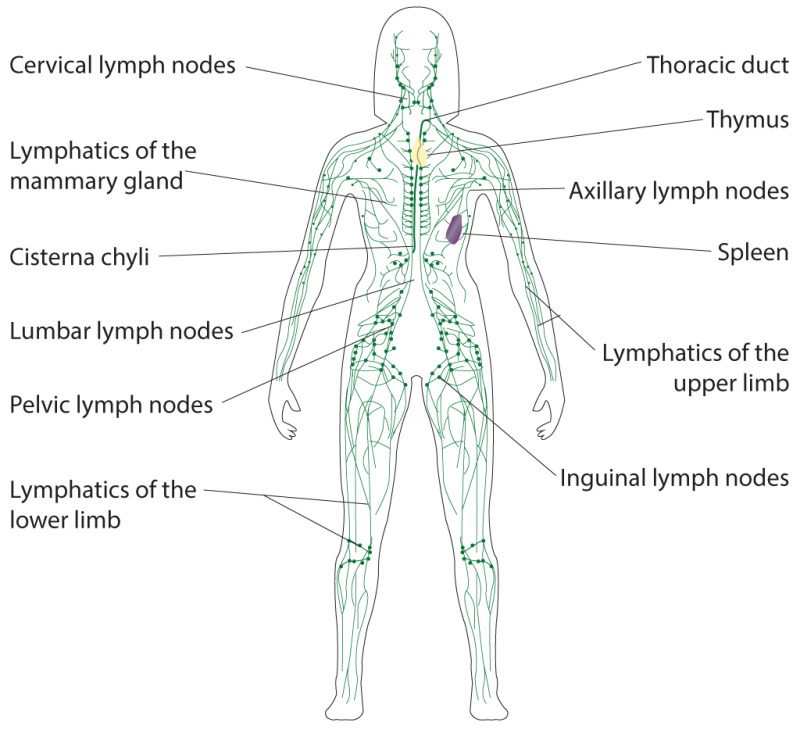
The lymphatic system, or lymphoid system, is one of the components of the circulatory system, and it serves a critical role in both immune function and surplus extracellular fluid drainage. (see Image. Lymphatic System). Components of the lymphatic system include lymph, lymphatic vessels and plexuses, lymph nodes, lymphatic cells, and a variety of lymphoid organs. The pattern and form of lymphatic channels are more variable and complex but generally parallel those of the peripheral vascular system. The lymphatic system partly functions to convey lymphatic fluid, or lymph, through a network of lymphatic channels, filter lymphatic fluid through lymph nodes and return lymphatic fluid to the bloodstream, where it is eventually eliminated. Nearly all body organs, regions, and systems have lymphatic channels to collect the various byproducts that require elimination (see Images. Axillary Lymph Nodes, Lymphatics of the Lower Limb). Liver and intestinal lymphatics produce about 80% of the volume of lymph in the body.[1]
Notable territories of the body that do not appear to contain lymphatics include the bone marrow, epidermis, as well as other tissues where blood vessels are absent. The central nervous system was long considered to be absent of lymphatic vessels until they were recently identified in the cranial meninges.[2][3] Moreover, a vessel appearing to have lymphatic features was also discovered in the eye.[4][5] The lymphatic system is critical in a clinical context, particularly given that it is a major route for cancer metastasis and that the inflammation of lymphatic vessels and lymph nodes is an indicator of pathology.
Structure
The lymphatic system includes numerous structural components, including lymphatic capillaries, afferent lymphatic vessels, lymph nodes, efferent lymphatic vessels, and various lymphoid organs.
Lymphatic capillaries are tiny, thin-walled vessels that originate blindly within the extracellular space of various tissues. Lymphatic capillaries tend to be larger in diameter than blood capillaries and are interspersed among them to enhance their ability to collect interstitial fluid efficiently. They are critical in the drainage of extracellular fluid and allow this fluid to enter the closed capillaries but not exit due to their unique morphology. Lymphatic capillaries at their blind ends are composed of a thin endothelium without a basement membrane. The endothelial cells at the closed end of the capillary overlap but shift to open the capillary end when interstitial fluid pressure is greater than intra-capillary pressure. This process permits lymphocytes, interstitial fluid, bacteria, cellular debris, plasma proteins, and other cells to enter the lymphatic capillaries. Special lymphatic capillaries called lacteals exist in the small intestine to contribute to the absorption of dietary fats. Lymphatics in the liver contribute to a specialized role in transporting hepatic proteins into the bloodstream.[1] The lymphatic capillaries of the body form large networks of channels called lymphatic plexuses and converge to form larger lymphatic vessels.
Lymphatic vessels convey lymph, or lymphatic fluid, through their channels. Afferent (toward) lymphatic vessels convey unfiltered lymphatic fluid from the body tissues to the lymph nodes, and efferent (away) lymphatic vessels convey filtered lymphatic fluid from lymph nodes to subsequent lymph nodes or into the venous system. The various efferent lymphatic vessels in the body eventually converge to form two major lymphatic channels: the right lymphatic duct and the thoracic duct.
The right lymphatic duct drains most of the right upper quadrant of the body, including the right upper trunk, right upper extremity, and right head and neck (see Image. Lymphatics of the Oral and Nasal Cavity). The right lymphatic trunk is a visible channel in the right cervical region just anterior to the anterior scalene muscle. Its origin and termination are variable in morphology, typically forming as the convergence of the right bronchomediastinal, jugular, and subclavian trunks, extending 1 to 2 centimeters in length before returning its contents to the systemic circulation at the junction of the right internal jugular, subclavian, and/or brachiocephalic veins.
The thoracic duct, also known as the left lymphatic duct or van Hoorne's canal, is the largest of the body's lymphatic channels. It drains most of the body except for the territory of the right superior thorax, head, neck, and upper extremity served by the right lymphatic duct. The thoracic duct is a thin-walled tubular vessel measuring 2 to 6 mm in diameter. The length of the duct ranges from 36 to 45 cm. The thoracic duct is highly variable in form but typically arises in the abdomen at the superior aspect of the cisterna chyli, around the level of the twelfth thoracic vertebra (T12). The cisterna chyli, from which it extends, is an expanded lymphatic sac that forms at the convergence of the intestinal and lumbar lymphatic trunks extending along the L1-L2 vertebral levels. The cisterna chyli is present in approximately 40-60% of the population, and in its absence, the intestinal and lumbar lymphatic trunks communicate directly with the thoracic duct at the T12 level.[6][7]
As a result, the thoracic duct receives lymphatic fluid from the lumbar lymphatic trunks and chyle, composed of lymphatic fluid and emulsified fats, from the intestinal lymphatic trunk. Initially, the thoracic duct is located just to the right of the midline and posterior to the aorta. It exits the abdomen and enters the thorax via the aortic hiatus formed by the right and left crura of the diaphragm, side by side with the aorta. The thoracic duct then ascends in the thoracic cavity just anterior and to the right of the vertebral column between the aorta and azygos vein. At about the level of the fifth thoracic vertebra (T5), the thoracic duct typically crosses to the left of the vertebral column and posterior to the esophagus. From here, it ascends vertically and usually empties its contents into the junction of the left subclavian and left internal jugular veins in the cervical region.
To ensure that lymph does not flow backward, collecting lymphatic vessels and larger lymphatic vessels have one-way valves. These valves are not present in the lymphatic capillaries. These lymphatic valves permit the continued advancement of lymph through the lymphatic vessels aided by a pressure gradient created by vascular smooth muscle, skeletal muscle contraction, and respiratory movements. However, it is important to note that lymphatic vessels also communicate with the venous system through various anastomoses.
Lymph nodes are small bean-shaped tissues situated along lymphatic vessels. Lymph nodes receive lymphatic fluid from afferent lymphatic vessels and convey lymph away through efferent lymphatic vessels. Lymph nodes serve as a filter and function to monitor lymphatic fluid/blood composition, drain excess tissue fluid and leaked plasma proteins, engulf pathogens, augment an immune response, and eradicate infection.
Several organs in the body are considered to be lymphoid or lymphatic organs, given their role in the production of lymphocytes. These include the bone marrow, spleen, thymus, tonsils, lymph nodes, and other tissues. Lymphoid organs can be categorized as primary or secondary lymphoid organs. Primary lymphoid organs are those that produce lymphocytes, such as the bone marrow and thymus. Bone marrow is the primary site for the production of lymphocytes. The thymus is a glandular organ located anterior to the pericardium. It serves to mature and develop T cells, or thymus cell lymphocytes, in response to an inflammatory process or pathology. As individuals age, both their bone marrow and thymus reduce and accumulate fat. Secondary lymphoid organs serve as territories in which immune cells function and include the spleen, tonsils, lymph nodes, and various mucous membranes, such as in the intestines. The spleen is a purplish, fist-sized organ in the left upper abdominal quadrant that contributes to immune function by serving as a blood filter, storing lymphocytes within its white pulp, and being a site for an adaptive immune response to antigens. The lingual tonsils, palatine tonsils, and pharyngeal tonsils, or adenoids, work to prevent pathogens from entering the body. Mucous membranes in the gastrointestinal, respiratory, and genitourinary systems also function to prevent pathogens from entering the body.
Lymph
Lymphatic fluid, or lymph, is similar to blood plasma and tends to be watery, transparent, and yellowish in appearance. Extracellular fluid leaks out of the blood capillary walls because of pressure exerted by the heart or osmotic pressure at the cellular level. As the interstitial fluid accumulates, it is picked up by the tiny lymphatic capillaries along with other substances to form lymph. This fluid then passes through the lymphatic vessels and lymph nodes and finally enters the venous circulation. As the lymph passes through the lymph nodes, both monocytes and lymphocytes enter it.
Lymph is composed primarily of interstitial fluid with variable amounts of lymphocytes, bacteria, cellular debris, plasma proteins, and other cells. In the GI tract, lymphatic fluid is called chyle and has a milk-like appearance that is chiefly due to the presence of cholesterol, glycerol, fatty acids, and other fat products. The vessels that transport the lymphatic fluid from the GI tract are known as lacteals.
Embryology
The development of the lymphatic system is known from both human and animal, especially mouse studies. The lymphatic vessels form after the development of blood vessels, around six weeks post-fertilization. The endothelial cells that serve as precursors to the lymphatics arise from the embryonic cardinal veins.[8] The process by which lymphatic vessels form is similar to that of the blood vessels and produces lymphatic-venous and intra-lymphatic anastomoses, but diverse origins exist for components of lymphatic vessel formation in different regions.[9][10][11][12]
Six primary lymph sacs develop and are apparent about eight weeks post-fertilization. These include, from caudal to cranial, one cisterna chyli, one retroperitoneal lymph sac, two iliac lymph sacs, and two jugular lymph sacs. The jugular lymph sacs are the first to develop, initially appearing next to the jugular part of the cardinal vein.[12] Lymphatic vessels then form adjacent to the blood vessels and connect the various lymph sacs. The lymphatic vessels primarily arise from the lymph sacs through the process of self-proliferation and polarized sprouting.[13]
Stem/progenitor cells play a huge role in forming lymphatic tissues and vessels by contributing to sustained growth and postnatally differentiating into lymphatic endothelial cells.[13] Lymphatic channels from the developing gut connect with the retroperitoneal lymph sac and the cisterna chyli, situated just posteriorly. The lymphatic channels of the lower extremities and inferior trunk communicate with the iliac lymph sacs. Finally, lymphatic channels in the head, neck and upper extremities drain to the jugular lymph sacs. Additionally, a right and left thoracic duct form and connect the cisterna chyli with the jugular lymph sacs and form anastomoses that eventually produce the typical adult form. The lymph sacs then produce groups of lymph nodes in the fetal period. Migrating mesenchyme enters the lymph sacs and produces lymphatic networks, connective tissue, and other layers of the lymph nodes.
Function
The lymphatic system's primary function is to balance the volume of interstitial fluid and convey it and excess protein molecules into the venous circulation.[14] The lymphatic system is also important in immune surveillance, defending the body against foreign particles and microorganisms. It does so by conveying antigens and leukocytes to lymph nodes, where antigen-primed and targeted lymphocytes and other immune cells are conveyed into the lymphatic vessels and blood vessels.[14] In addition, the system has a role in the absorption of fat-soluble vitamins and fatty substances in the gut via the gastrointestinal tract's lacteals within the villi and the transport of this material into the venous circulation.[15]
Newly recognized lymphatic vessels are visible in the meninges relating to cerebrospinal fluid (CSF) outflow from the central nervous system.[2][3] Finally, lymphatics may play a role in the clearance of ocular fluid via the lymphatic-like Schlemm canals.[4][5]
Clinical Significance
Leaks of lymphatic fluid occur when the lymphatic vessels are damaged. In the abdomen, lymphatic vessel damage may occur during surgery, especially during retroperitoneal procedures such as repairing an abdominal aortic aneurysm. These leaks tend to be mild, and the vessels in the peritoneum and mesentery eventually absorb the lymphatic fluid or chyle. However, when the thoracic duct is injured in the chest, the chyle leak can be extensive. In most cases, conservative care with a no-fat diet (medium chain triglycerides) or total parenteral nutrition is unsuccessful. In most cases, if the injury to the thoracic duct was surgical, a surgical procedure is required to tie off the duct. If the thoracic duct is injured in the cervical region, then inserting a drainage tube and adopting a low-fat diet will help seal the leak. However, thoracic duct injury in the chest cavity usually requires drainage and surgery. It is rare for the thoracic segment of the thoracic duct to seal on its own.[16][17][18]
In terms of accumulation of chyle in the thorax (i.e., chylothorax), if a patient has an injury to the thoracic duct in the thorax below the T5 vertebral level, then fluid will collect in only the right pleural cavity. If the injury is to the thoracic duct in the thorax above the T5 vertebral level, then fluid will appear in both pleural cavities.
Other Issues
The lymphatic system is prone to disorders like the venous and arterial circulatory systems. Developmental or functional defects of the lymphatic system cause lymphedema. When this occurs, the lymphatic system is unable to sufficiently drain lymphatic fluid resulting in its accumulation and swelling of the territory. Lymphedema, this swelling due to the accumulation of lymph, is classified as primary or secondary.
Primary lymphedema is an inherited disorder where the lymphatic system development has been disrupted, causing absent or malformed lymphatic tissues. This condition often presents soon after birth, but some conditions may present later in life (e.g., at puberty or later adulthood). There are no effective treatments for primary lymphedema. Past surgical treatments were found to be mutilating and are no longer implemented. The present-day treatment revolves around compression stockings, pumps, and constrictive garments.[19][20][21]
Secondary lymphedema is an acquired disorder involving lymphatic system dysfunction that may result from many causes, including cancer, infection, trauma, or surgery. The treatment of secondary lymphedema depends on the cause. Oncological and other surgeries may result in secondary lymphedema due to the removal or biopsy of lymph nodes or lymphatic vessels. Non-surgical lymphedema may result from malignancies, obstruction within the lymphatic system, infection, or deep vein thrombosis. In most cases of obstructive secondary lymphedema, the drainage will resume if the inciting cause is removed, although some individuals may need to wear compressive stockings permanently. Also, physical therapy may help alleviate lymphedema when the extremities are involved. There is no absolute cure for lymphedema, but diagnosis and careful management can help to minimize complications.[22]
Lymphomas are cancers that arise from the cells of the lymphatic system. There are numerous types of lymphoma, but they are grouped into Hodgkin lymphoma and non-Hodgkin lymphoma.[23] Lymphomas usually arise from the malignant transformation of specific lymphocytes in the lymphatic vessels or lymph nodes in the gastrointestinal tract, neck, axilla, or groin. Symptoms of lymphoma may include night sweats, fever, fatigue, itching, and weight loss.
Cancers originating outside of the lymphatic system often spread via the lymphatic vessels and may involve regional lymph nodes serving the impacted organs or tissues.
Lymphadenitis occurs when the lymph nodes become inflamed or enlarged. The cause is usually an adjacent bacterial infection but may also involve viruses or fungi. The lymph nodes usually enlarge and become tender.
Lymphatic filariasis, or elephantiasis, is a very common mosquito-borne disorder caused by a parasite found in tropical and subtropical areas of the world, including Africa, Asia, the Pacific, the Caribbean, and South America. This condition involves parasitic microscopic nematodes (roundworms) that infect the lymphatic system and rapidly multiply and disrupt lymphatic function.[24] Many infected individuals may have no outward symptoms, although the kidneys and lymphatic tissues may be damaged and dysfunctional. Symptomatic individuals may present with disfigurement caused by significant lymphedema and elephantiasis (thickening of the skin, particularly the extremities). The parasite may also cause hydrocele, an enlargement of the scrotum due to the accumulation of fluid, which may result from obstruction of the lymph nodes or vessels in the groin. Individuals presenting with symptoms have poorly draining lymphatics, often involving the extremities, resulting in huge extremities and marked disability. Lymphatic filariasis is the most common cause of disfigurement in the world, and it is the second most common cause of long-term disability.[24]
Enhancing Healthcare Team Outcomes
All interprofessional healthcare team members need to understand the function and significance of the lymphatic system since it participates in or can be implicated in many disease states. Clinicians (MDs, DOs, NPOs, and PAs) are most in need of a thorough understanding, but nurses, pharmacists, and other ancillary healthcare team members should also comprehend the basic anatomy and physiology of the lymphatic system and how it can relate to various disease states.


Figure
Lymphatics of the Oral and Nasal Cavity. Illustrated anatomy includes the parotid glands, superficial cervical glands, deep cervical glands, submaxillary glands, and facial glands. Henry Vandyke Carter, Public Domain, via Wikimedia Commons


Figure
Lymphatics of the Lower Limb. Illustrated image includes the superficial inguinal and subinguinal glands. Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
- 1.
- Hsu MC, Itkin M. Lymphatic Anatomy. Tech Vasc Interv Radiol. 2016 Dec;19(4):247-254. [PubMed: 27993319]
- 2.
- Louveau A, Smirnov I, Keyes TJ, Eccles JD, Rouhani SJ, Peske JD, Derecki NC, Castle D, Mandell JW, Lee KS, Harris TH, Kipnis J. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015 Jul 16;523(7560):337-41. [PMC free article: PMC4506234] [PubMed: 26030524]
- 3.
- Aspelund A, Antila S, Proulx ST, Karlsen TV, Karaman S, Detmar M, Wiig H, Alitalo K. A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. J Exp Med. 2015 Jun 29;212(7):991-9. [PMC free article: PMC4493418] [PubMed: 26077718]
- 4.
- Kizhatil K, Ryan M, Marchant JK, Henrich S, John SW. Schlemm's canal is a unique vessel with a combination of blood vascular and lymphatic phenotypes that forms by a novel developmental process. PLoS Biol. 2014 Jul;12(7):e1001912. [PMC free article: PMC4106723] [PubMed: 25051267]
- 5.
- Aspelund A, Tammela T, Antila S, Nurmi H, Leppänen VM, Zarkada G, Stanczuk L, Francois M, Mäkinen T, Saharinen P, Immonen I, Alitalo K. The Schlemm's canal is a VEGF-C/VEGFR-3-responsive lymphatic-like vessel. J Clin Invest. 2014 Sep;124(9):3975-86. [PMC free article: PMC4153703] [PubMed: 25061878]
- 6.
- KAUSEL HW, REEVE TS, STEIN AA, ALLEY RD, STRANAHAN A. Anatomic and pathologic studies of the thoracic duct. J Thorac Surg. 1957 Nov;34(5):631-41. [PubMed: 13476471]
- 7.
- Phang K, Bowman M, Phillips A, Windsor J. Review of thoracic duct anatomical variations and clinical implications. Clin Anat. 2014 May;27(4):637-44. [PubMed: 24302465]
- 8.
- Wigle JT, Oliver G. Prox1 function is required for the development of the murine lymphatic system. Cell. 1999 Sep 17;98(6):769-78. [PubMed: 10499794]
- 9.
- Stone OA, Stainier DYR. Paraxial Mesoderm Is the Major Source of Lymphatic Endothelium. Dev Cell. 2019 Jul 22;50(2):247-255.e3. [PMC free article: PMC6658618] [PubMed: 31130354]
- 10.
- Klotz L, Norman S, Vieira JM, Masters M, Rohling M, Dubé KN, Bollini S, Matsuzaki F, Carr CA, Riley PR. Cardiac lymphatics are heterogeneous in origin and respond to injury. Nature. 2015 Jun 04;522(7554):62-7. [PMC free article: PMC4458138] [PubMed: 25992544]
- 11.
- Stanczuk L, Martinez-Corral I, Ulvmar MH, Zhang Y, Laviña B, Fruttiger M, Adams RH, Saur D, Betsholtz C, Ortega S, Alitalo K, Graupera M, Mäkinen T. cKit Lineage Hemogenic Endothelium-Derived Cells Contribute to Mesenteric Lymphatic Vessels. Cell Rep. 2015 Mar 17;10(10):1708-1721. [PubMed: 25772358]
- 12.
- Mäkinen T, Boon LM, Vikkula M, Alitalo K. Lymphatic Malformations: Genetics, Mechanisms and Therapeutic Strategies. Circ Res. 2021 Jun 25;129(1):136-154. [PubMed: 34166072]
- 13.
- Mou R, Chen K, Zhu P, Xu Q, Ma L. The Impact of Stem/Progenitor Cells on Lymphangiogenesis in Vascular Disease. Cells. 2022 Dec 15;11(24) [PMC free article: PMC9776475] [PubMed: 36552820]
- 14.
- Petrova TV, Koh GY. Biological functions of lymphatic vessels. Science. 2020 Jul 10;369(6500) [PubMed: 32646971]
- 15.
- Zemmez Y, Boui M. [Elephantiasis of the left lower limb]. Pan Afr Med J. 2018;29:95. [PMC free article: PMC5987132] [PubMed: 29875976]
- 16.
- Ilahi M, St Lucia K, Ilahi TB. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 24, 2023. Anatomy, Thorax, Thoracic Duct. [PubMed: 30020599]
- 17.
- Ohkura Y, Ueno M, Shindoh J, Iizuka T, Ka H, Udagawa H. Risk Factors for Postoperative Chylothorax After Radical Subtotal Esophagectomy. Ann Surg Oncol. 2018 Sep;25(9):2739-2746. [PubMed: 29998406]
- 18.
- Glatz T, Marjanovic G, Hoeppner J. [Prevention and Surgical Therapy of Chylothorax]. Zentralbl Chir. 2018 Jun;143(3):278-283. [PubMed: 29933480]
- 19.
- Kilarski WW. Physiological Perspective on Therapies of Lymphatic Vessels. Adv Wound Care (New Rochelle). 2018 Jul 01;7(7):189-208. [PMC free article: PMC6032671] [PubMed: 29984111]
- 20.
- Granzow JW. Lymphedema surgery: the current state of the art. Clin Exp Metastasis. 2018 Aug;35(5-6):553-558. [PubMed: 29980891]
- 21.
- Rooney L, Cooper-Stanton G, Cave-Senior J. Compression therapy and exercise: enhancing outcomes. Br J Community Nurs. 2018 Jul 02;23(7):343-346. [PubMed: 29972671]
- 22.
- Sleigh BC, Manna B. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Apr 19, 2023. Lymphedema. [PubMed: 30725924]
- 23.
- Matasar MJ, Zelenetz AD. Overview of lymphoma diagnosis and management. Radiol Clin North Am. 2008 Mar;46(2):175-98, vii. [PubMed: 18619375]
- 24.
- Lourens GB, Ferrell DK. Lymphatic Filariasis. Nurs Clin North Am. 2019 Jun;54(2):181-192. [PubMed: 31027660]
Disclosure: Manda Null declares no relevant financial relationships with ineligible companies.
Disclosure: Tafline Arbor declares no relevant financial relationships with ineligible companies.
Disclosure: Manuj Agarwal declares no relevant financial relationships with ineligible companies.
Publication Details
Author Information and Affiliations
Authors
Manda Null1; Tafline C. Arbor2; Manuj Agarwal3.Affiliations
Publication History
Last Update: March 6, 2023.
Copyright
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
Publisher
StatPearls Publishing, Treasure Island (FL)
NLM Citation
Null M, Arbor TC, Agarwal M. Anatomy, Lymphatic System. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.