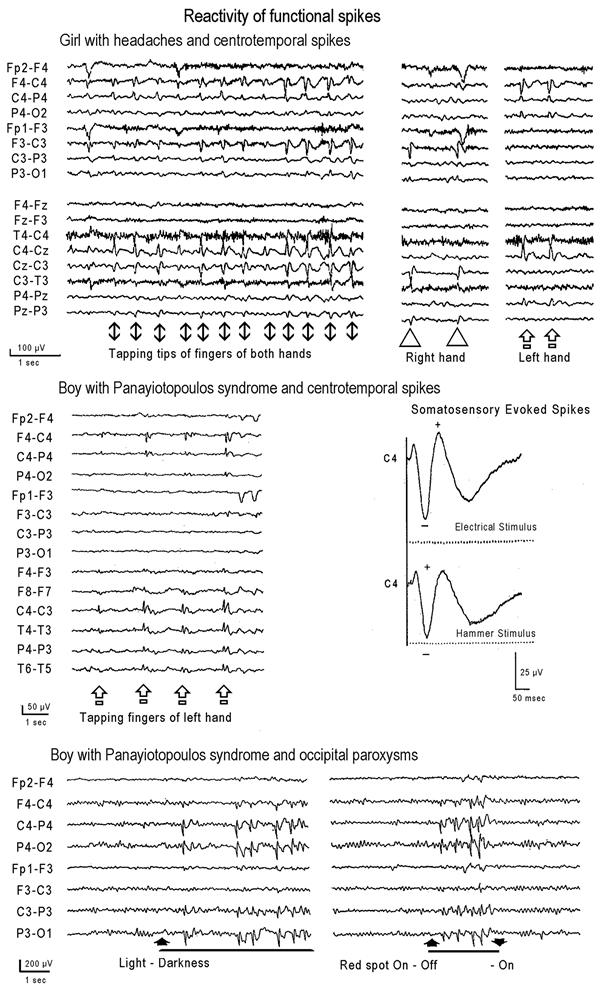
Activation of functional centrotemporal and occipital spikes. Facing page
Top: Video EEG of a 6-year-old girl with headaches and abdominal
pains of recent onset (case 16.2 in ref1).
Neurological examination and MRI were normal. Symptoms improved over the following
year. She never had seizures and her development was normal. EEG showed normal
background with the following abnormalities:
(a). Spontaneously central spikes, occurring independently on the right or left.
(b). High amplitude central spikes elicited by somatosensory stimulation of the
contralateral side. Simultaneous stimulation of the fingers of the hands by the
patient herself elicited simultaneous bilateral central spikes.
(c). Brief, mainly anterior, bursts of polyspikes.
(d). Brief and high amplitude generalised discharges of 3–5 Hz slow
waves interspersed with small spikes or small polyspikes.
Note that the ESES are bilateral and synchronous when the stimulus is also
bilateral and synchronous (tapping together and simultaneously the palmar tips of
her fingers). Unilateral tapping evoked contralateral ESES.
Middle: ESES of a patient with PS (case 17 in ref4). At the age of 8 years, this boy had a
single nocturnal seizure, which started with repetitive vomiting and “he
was lost”. He then clenched his teeth and became rigid, but there were
no clonic convulsions. The last follow-up, at the age of 14 years, disclosed no
further seizures and normal development, though school performance was moderate.
Three EEGs showed right CTS that were also evoked by somatosensory stimuli.
Occipital spikes were never observed.
Bottom: Sample EEG from a patient with PS and occipital paroxysms
(case 6 in ref4). Occipital paroxysms are
bilateral and synchronous, because they are activated in the hyperexcitable
occipital cortices by the elimination of central vision and fixation.