

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
National Guideline Centre (UK). Venous thromboembolism in over 16s: Reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism. London: National Institute for Health and Care Excellence (NICE); 2018 Mar. (NICE Guideline, No. 89.)

December 2019: In recommendation 1.3.5 the British Standards for anti-embolism hosiery were updated because BS 6612 and BS 7672 have been withdrawn. August 2019: Recommendation 1.12.11 (1.5.30 in this document) was amended to clarify when anti-embolism stockings can be used for VTE prophylaxis for people with spinal injury.
Venous thromboembolism in over 16s: Reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism.
Show detailsM.1. Network meta-analysis for elective hip replacement surgery
M.1.1. Introduction
The results of conventional meta-analyses of direct evidence alone (as presented in the GRADE profiles in appendix K and forest plots in appendix L) does not help inform which intervention is most effective as VTE prophylaxis in patients undergoing elective hip replacement surgery. The challenge of interpretation has arisen for two reasons:
- In isolation, each pair-wise comparison does not inform the choice among the different treatments; in addition direct evidence is not available for some pair-wise comparisons in a randomised controlled trial.
- There are frequently multiple overlapping comparisons that could potentially give inconsistent estimates of effect.
To overcome these problems, a hierarchical Bayesian network meta-analysis (NMA) was performed. This type of analysis allows for the synthesis of data from direct and indirect comparisons without breaking randomisation and allows for the ranking of different interventions. In this case the outcomes were defined as:
- Deep vein thrombosis (DVT; symptomatic and asymptomatic)
- Major bleeding
The analysis also provided estimates of effect (with 95% credible intervals) for each intervention compared to one another and compared to a single baseline risk (in this case the baseline treatment was no prophylaxis or in the case of the major bleeding outcome a combination of no prophylaxis and mechanical prophylaxis). These estimates provide a useful clinical summary of the results and facilitate the formation of recommendations based on the best available evidence.
Conventional fixed effects meta-analysis assumes that the relative effect of one treatment compared to another is the same across an entire set of trials. In a random effects model, it is assumed that the relative effects are different in each trial but that they are from a single common distribution and that this distribution is common across all sets of trials.
Network meta-analysis requires an additional assumption over conventional meta-analysis. The additional assumption is that intervention A has the same effect on people in trials of intervention A compared to intervention B as it does for people in trials of intervention A versus intervention C, and so on. Thus, in a random effects network meta-analysis, the assumption is that intervention A has the same effect distribution across trials of A versus B, A versus C and so on.
This specific method is usually referred to as mixed-treatment comparisons analysis but we will continue to use the term network meta-analysis to refer generically to this kind of analysis. We do so since the term “network” better describes the data structure, whereas “mixed treatments” could easily be misinterpreted as referring to combinations of treatments.
M.1.2. Methods
M.1.2.1. Study selection
To estimate the relative risks, we performed an NMA that simultaneously used all the relevant RCT evidence from the clinical evidence review. As with conventional meta-analyses, this type of analysis does not break the randomisation of the evidence, nor does it make any assumptions about adding the effects of different interventions. The effectiveness of a particular treatment strategy combination will be derived only from randomised controlled trials that had that particular combination in a trial arm.
M.1.2.2. Outcome measures
The NMA evidence reviews for interventions considered three clinical efficacy outcomes identified from the clinical evidence review; number of people with DVT, number of people with PE and number of people with major bleeding. Other outcomes were not considered for the NMA as they were infrequently reported across the studies. The guideline committee considered that these outcomes were the most critical clinical outcomes for testing effectiveness of VTE prophylaxis.
M.1.2.3. Comparability of interventions
The interventions compared in the model were those found in the randomised controlled trials and included in the clinical evidence review already presented in Chapter 26 of the full guideline and in appendix H. If an intervention was evaluated in a study that met the inclusion criteria for the network (that is if it reported at least one of the outcomes of interest and matched the inclusion criteria for the meta-analysis) then it was included in the network meta-analysis, otherwise it was excluded.
The treatments included in each network are shown in Table 237.
Table 237Treatments included in network meta-analysis
|
Network 1: Number of people with DVT |
Network 2: Number of people with PE |
Network 3: Number of people with major bleeding |
|---|---|---|
| No prophylaxis | No prophylaxis | No prophylaxis/mechanical |
| LMWH (standard dose; standard duration) | LMWH (standard dose; standard duration) | UFH (standard duration) |
| UFH (standard duration) | LMWH (standard dose) + AES | LMWH (high dose; standard duration) |
| LMWH (standard dose) + AES | IPCD (length unspecified) | LMWH (standard dose; standard duration) |
| LMWH (high dose; standard duration) | UFH (standard duration) | Fondaparinux |
| IPCD | Rivaroxaban | LMWH (low dose; post-op) |
| LMWH (standard dose; extended duration) | LMWH (standard dose; extended duration) | VKA (standard duration) |
| Dabigatran | LMWH (high dose; standard duration) | Dabigatran |
| Foot pump | Dabigatran | Apixaban |
| Apixaban | Foot pump | Rivaroxaban |
| Rivaroxaban | Apixaban | LMWH (standard dose; extended duration) |
| VKA (standard duration) | AES (length unspecified) | LMWH (low dose; pre-op) |
| UFH (extended duration) | LMWH (low dose) + AES | VKA (extended duration) |
| Aspirin | Fondaparinux + AES | LMWH (standard dose; standard duration) followed by aspirin (extended duration) |
| LMWH (low dose) + AES | LMWH (standard dose; extended duration) + AES | LMWH (high dose; extended duration) |
| LMWH (extended duration) + AES | Aspirin (standard duration) | - |
| Fondaparinux + AES | LMWH (standard dose; standard duration) followed by aspirin (extended duration) | - |
| AES (length unspecified) | VKA (standard duration) | - |
| LMWH (low dose; pre-op) | UFH + AES | - |
| LMWH (low dose; post-op) | AES (above-knee) | - |
| VKA (extended duration) | LMWH (high dose) + AES | - |
| AES (above-knee) | VKA (extended duration) | - |
| LMWH (high dose) + AES | LMWH (high dose; extended duration) | |
| UFH + AES | - | - |
| Foot pump + AES | - | - |
| LMWH (high dose; extended duration) | - |
M.1.2.4. Baseline risks
The baseline risk is defined as the risk of achieving the outcome of interest in the baseline treatment arm of the included trials. This figure is useful because it allows us to convert the results of the NMA from odds ratios to relative risks. However, the majority of the trials were old studies that reported very high risk of DVT and PE in the no prophylaxis arm that the orthopaedic subgroup considered to be not reflective of the baseline risk in the UK. Hence, for the purpose of calculating the relative risks of these events for presentation in this appendix, the baseline risk values were obtained from a large observational study that used data from the UK National Joint Registry (NJR).451 For full details please refer to HE write-up (appendix P, section P.1.3.3).
M.1.2.5. Statistical analysis
A hierarchical Bayesian network meta-analysis (NMA) was performed using the software WinBUGS. We adapted a three-arm random effects model template for the networks, from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). This model accounts for the correlation between study level effects induced by multi-arm trials.
In order to be included in the analysis, a fundamental requirement is that each treatment is connected directly or indirectly to every other intervention in the network. For each outcome subgroup, a diagram of the evidence network is presented in section M.1.3.
The model used was a random effects logistic regression model, with parameters estimated by Markov chain Monte Carlo simulation. As it was a Bayesian analysis, for each parameter the evidence distribution is weighted by a distribution of prior beliefs. Due to the sparse nature of the networks (few studies per direct treatment comparison), the between-study heterogeneity parameter is imprecisely estimated in a random effects model. Therefore it is beneficial to apply informative priors in order to restrict the prior distribution for heterogeneity to avoid unreasonably wide credible intervals. Turner et al (2015)946 derived a novel set of predictive distributions for the degree of heterogeneity across 80 different settings. Appropriate predictive distributions for heterogeneity were chosen from Turner et al (2015)946 and used directly as informative priors. The log normal (µ, ơ2) predictive distributions obtained for the between-study heterogeneity in a future meta-analysis presented in Table IV946 were selected according to the outcome and treatment comparison. For the DVT and PE NMAs the distributions defined by the outcome of “general physical health indicators” and by the intervention/comparison type “non-pharmacological vs. pharmacological” were chosen (LN[−1.26, 1.252]). For the major bleeding NMA the distributions defined by the outcome of “adverse events” and by the intervention/comparison type “non-pharmacological vs. pharmacological” were chosen (LN[−0.84, 1.242]). These distributions were chosen as they represented outcomes measured by an assessor, whose method of measurement as well as judgement may influence the outcome (as studies provided slightly variable ways of defining these critical outcomes), and the interaction aspect encompassed both the pharmacological and mechanical prophylaxis options covered in our review protocol.
For the analyses, a series of 60,000 burn-in simulations were run to allow convergence and then a further 60,000 simulations were run to produce the outputs. Convergence was assessed by examining the history and kernel density plots.
We tested the goodness of fit of the model by calculating the residual deviance. If the residual deviance is close to the number of unconstrained data points (the number of trial arms in the analysis) then the model is explaining the data well.
The results, in terms of relative risk, of pair-wise meta-analyses are presented in the clinical evidence review (Chapter 26, and appendix H).
The aim of the NMA was to calculate treatment specific log odds ratios and relative risks for response to be consistent with the comparative effectiveness results presented elsewhere in the clinical evidence review and for ease of interpretation. Let BO, , and p denote the baseline odds, treatment specific odds, treatment specific log odds ratio and treatment specific absolute probability respectively. Then:
And:
Once the treatment specific probabilities for response are calculated, we divide them by the baseline probability (pb) to get treatment specific relative risks (rrb):
This approach has the advantage that baseline and relative effects are both modelled on the same log odds scale, and also ensures that the uncertainty in the estimation of both baseline and relative effects is accounted for in the model.
We also calculated the overall ranking of interventions according to their relative risk compared to control group. Due to the skewness of the data, the NMA relative risks and rank results are reported as medians rather than means (as in the direct comparisons) to give a more accurate representation of the ‘most likely’ value. The median rank for each intervention was derived from the resulting distribution and these are presented on a rank plot with the associated 95% credible intervals.
A key assumption behind NMA is that the network is consistent. In other words, it is assumed that the direct and indirect treatment effect estimates do not disagree with one another. Discrepancies between direct and indirect estimates of effect may result from several possible causes. First, there is chance and if this is the case then the network meta-analysis results are likely to be more precise as they pool together more data than conventional meta-analysis estimates alone. Second, there could be differences between the trials included in terms of their clinical or methodological characteristics.
This heterogeneity is a problem for network meta-analysis but may be dealt with by subgroup analysis, meta-regression or by carefully defining inclusion criteria. Inconsistency, caused by heterogeneity, was assessed subjectively by comparing the relative risks from the direct evidence (from pair-wise meta-analysis) to the relative risks from the combined direct and indirect evidence (from NMA). We further tested for inconsistency by developing inconsistency models for networks of binary outcomes using the TSD 4 template from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). We compared the posterior mean of the residual deviance between the consistency and inconsistency models to see which was a better fit to the data (closest to the number of trial arms in each network) and checked the difference in deviance information criterion (DIC) values between the two models was small (less than 3–5) or if it was larger, that the smaller DIC and hence better fitting model was the consistency model. No inconsistency was identified.
M.1.3. Results
M.1.3.1. Deep vein thrombosis (symptomatic and asymptomatic)
Included studies
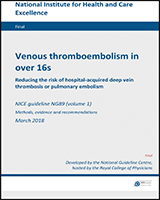
44 studies were identified as reporting on DVT outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 42 studies involving 26 treatments were included in the network for DVT (symptomatic and asymptomatic). The network can be seen in Figure 827 and the trial data for each of the studies included in the NMA are presented in Table 238.
.&p=BOOKS&id=561788_appmf1.jpg "Click on image to zoom")
Figure 827Network diagram for DVT (symptomatic and asymptomatic)
Table 238Study data for DVT network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Comparison | Intervention 1 | Intervention 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | ||||
| Kalodiki 1996472 | No prophylaxis | LMWH (standard dose; standard duration) | LMWH (standard dose) + AES | 13 | 14 | 12 | 32 | 8 | 32 |
| Bergqvist 1996B92 | No prophylaxis | LMWH (standard dose; standard duration) | - | 43 | 116 | 21 | 117 | - | - |
| Tørholm 1991941 | No prophylaxis | LMWH (standard dose; standard duration) | - | 19 | 54 | 9 | 58 | - | - |
| Hampson 1974382 | No prophylaxis | UFH (standard duration) | - | 28 | 52 | 22 | 48 | - | - |
| Mannucci 1976604 | No prophylaxis | UFH (standard duration) | - | 36 | 75 | 14 | 68 | - | - |
| Turpie 1986952 | No prophylaxis | LMWH (high dose; standard duration) | - | 20 | 39 | 4 | 37 | - | - |
| Hull 1990 | No prophylaxis | IPCD (length unspecified) | - | 36 | 152 | 77 | 158 | - | - |
| Gallus 1983334 | No prophylaxis | IPCD (length unspecified) | - | 25 | 47 | 15 | 43 | - | - |
| Colwell 1994204 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 28 | 136 | 21 | 142 | 8 | 136 |
| Avikainen 199557 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 1 | 79 | 4 | 79 | - | - |
| Eriksson 1991A289 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 19 | 63 | 25 | 59 | - | - |
| Planes 1990A (Trial3)758 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 15 | 120 | 27 | 106 | - | - |
| Planes 1990A (Trial1)758 | LMWH (standard dose; standard duration) | LMWH (high dose; standard duration) | - | 12 | 150 | 5 | 78 | - | - |
| Hardwick 2011389 | LMWH (standard dose; standard duration) | IPCD (length unspecified) | - | 8 | 190 | 8 | 196 | - | - |
| Comp 2001209 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 39 | 138 | 15 | 152 | - | - |
| Lassen 1998528 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 12 | 102 | 5 | 113 | - | - |
| Planes 1996757 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 17 | 88 | 6 | 85 | - | - |
| Eriksson 2011292 | LMWH (standard dose; standard duration) | Dabigatran | - | 67 | 783 | 60 | 791 | - | - |
| Eriksson 2007288 | LMWH (standard dose; standard duration) | Dabigatran | - | 57 | 897 | 45 | 880 | - | - |
| Warwick 1998994 | LMWH (standard dose; standard duration) | Foot pump | - | 18 | 138 | 24 | 136 | - | - |
| Lassen 2010535 | LMWH (standard dose; standard duration) | Apixaban | - | 68 | 1911 | 22 | 1944 | - | - |
| Kakkar 2008467 | LMWH (standard dose; standard duration) | Rivaroxaban | - | 71 | 869 | 14 | 864 | - | - |
| Francis 1997A315 | LMWH (standard dose; standard duration) | VKA (standard duration) | - | 49 | 190 | 28 | 192 | - | - |
| Kakkar 2000468 | UFH (standard duration) | LMWH (high dose; standard duration) | - | 24 | 116 | 9 | 101 | - | - |
| Levine 1991551 | UFH (standard duration) | LMWH (high dose; standard duration) | - | 61 | 263 | 50 | 258 | - | - |
| Manganelli 1998601 | UFH (standard duration) | UFH (extended duration) | - | 4 | 33 | 6 | 28 | - | - |
| Zanasi 19881039 | UFH (standard duration) | Aspirin | - | 10 | 25 | 7 | 19 | - | - |
| Fuji 2008A328 | LMWH (standard dose) + AES | LMWH (low dose) + AES | AES (length unspecified) | 27 | 80 | 21 | 81 | 36 | 86 |
| Dahl 1997226 | LMWH (standard dose) + AES | LMWH (extended duration) + AES | - | 33 | 104 | 22 | 114 | - | - |
| Lassen 2002526 | LMWH (standard dose) + AES | Fondaparinux + AES | - | 83 | 918 | 36 | 908 | - | - |
| Samama 1997844 | LMWH (standard dose) + AES | AES (length unspecified) | - | 11 | 78 | 28 | 75 | - | - |
| Warwick 1995A996 | LMWH (standard dose) + AES | AES (length unspecified) | - | 22 | 78 | 33 | 78 | - | - |
| Paeiment 1987722 | IPCD (length unspecified) | VKA (standard duration) | - | 11 | 66 | 12 | 72 | - | - |
| Lassen 1991529 | AES (above-knee) | LMWH (low dose) + AES | - | 53 | 1558 | 12 | 1595 | - | - |
| Eriksson 2008291 | LMWH (standard dose; extended duration) | Rivaroxaban | - | 81 | 338 | 36 | 337 | 44 | 336 |
| Hull 2000440 | VKA (standard duration) | LMWH (low dose; pre-op) | LMWH (low dose; post-op) | 8 | 176 | 3 | 184 | - | - |
| Prandoni 2002771 | VKA (standard duration) | VKA (extended duration) | - | 29 | 93 | 44 | 97 | - | - |
| Turpie 2002K954 | Fondaparinux + AES | LMWH (high dose) + AES | - | 44 | 784 | 65 | 796 | - | - |
| Moskovitz 1978657 | AES (length unspecified) | UFH + AES | - | 19 | 28 | 8 | 32 | - | - |
| Fordyce 1992312 | AES (length unspecified) | Foot pump + AES | 4 | 39 | 16 | 40 | - | - | |
| Samama 2002845 | LMWH (high dose; extended duration) | VKA (extended duration) | - | 20 | 636 | 15 | 643 | - | - |
| Santori 1994850 | UFH + AES | Foot pump + AES | 23 | 65 | 9 | 67 | - | - | |
N; number of events, NA; number analysed
NMA results
Table 239 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 239Risk ratios for DVT (symptomatic and asymptomatic)
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no prophylaxis | LMWH (standard dose; standard duration) | 0.46 (0.33, 0.63) | 0.46 (0.23, 0.81) |
| UFH (standard duration) | 0.61 (0.45, 0.85) | 0.60 (0.28, 1.03) | |
| LMWH (standard dose) + AES | 0.27 (0.15, 0.50) | 0.14 (0.07, 0.59) | |
| LMWH (high dose; standard duration) | 0.21 (0.08, 0.56) | 0.28 (0.10, 0.67) | |
| IPCD | 0.53 (0.40, 0.69) | 0.80 (0.34, 1.41) | |
| LMWH (standard dose; extended duration) | - | 0.19 (0.05, 0.57) | |
| Dabigatran | - | 0.40 (0.11, 1.05) | |
| Foot pump | - | 0.62 (0.11, 1.83) | |
| Apixaban | - | 0.16 (0.03, 0.76) | |
| Rivaroxaban | - | 0.06 (0.01, 0.29) | |
| VKA (standard duration) | - | 0.44 (0.11, 1.13) | |
| UFH (extended duration) | - | 0.96 (0.15, 2.92) | |
| Aspirin | - | 0.54 (0.07, 1.87) | |
| LMWH (low dose) + AES | - | 0.13 (0.02, 0.89) | |
| LMWH (extended duration) + AES | - | 0.08 (0.01, 0.61) | |
| Fondaparinux + AES | - | 0.07 (0.01, 0.49) | |
| AES (length unspecified) | - | 0.30 (0.08, 1.46) | |
| LMWH (low dose; pre-op) | - | 0.19 (0.02, 1.00) | |
| LMWH (low dose; post-op) | - | 0.23 (0.03, 1.12) | |
| VKA (extended duration) | - | 0.16 (0.01, 1.08) | |
| AES (above-knee) | - | 0.23 (0.02, 2.04) | |
| LMWH (high dose) + AES | - | 0.10 (0.01, 1.07) | |
| UFH + AES | 0.27 (0.04, 1.82) | ||
| Foot pump + AES | - | 0.32 (0.04, 2.11) | |
| LMWH (high dose; extended duration) | 0.12 (0.00, 1.20) | ||
| Versus LMWH (standard dose; standard duration) | UFH (standard duration) | 1.27 (0.95, 1.70)* | 1.28 (0.72, 2.36) |
| LMWH (standard dose) + AES | 0.67 (0.32, 1.41)* | 0.33 (0.10, 1.65) | |
| LMWH (high dose; standard duration) | 0.40 (0.22, 0.72)* | 0.61 (0.26, 1.28) | |
| IPCD | 0.97 (0.37, 2.53)* | 1.67 (0.77, 3.74) | |
| LMWH (standard dose; extended duration) | 0.36 (0.23, 0.55) | 0.41 (0.16, 0.95) | |
| Dabigatran | 0.85 (0.66, 1.09)* | 0.87 (0.30, 2.06) | |
| Foot pump | 1.35 (0.77, 2.38)* | 1.30 (0.29, 4.12) | |
| Apixaban | 0.32 (0.20, 0.51)* | 0.36 (0.07, 1.43) | |
| Rivaroxaban | 0.20 (0.11, 0.35)* | 0.14 (0.04, 0.51) | |
| VKA (standard duration) | 0.57 (0.37, 0.86)* | 0.94 (0.29, 2.52) | |
| UFH (extended duration) | - | 1.97 (0.35, 7.54) | |
| Aspirin | - | 1.15 (0.17, 4.55) | |
| LMWH (low dose) + AES | - | 0.28 (0.04, 2.39) | |
| LMWH (extended duration) + AES | - | 0.18 (0.02, 1.61) | |
| Fondaparinux + AES | - | 0.14 (0.02, 1.31) | |
| AES (length unspecified) | - | 0.66 (0.14, 4.01) | |
| LMWH (low dose; pre-op) | - | 0.41 (0.05, 2.13) | |
| LMWH (low dose; post-op) | - | 0.50 (0.07, 2.46) | |
| VKA (extended duration) | - | 0.34 (0.03, 2.37) | |
| AES (above-knee) | - | 0.50 (0.07, 5.45) | |
| LMWH (high dose) + AES | - | 0.21 (0.02, 2.79) | |
| UFH + AES | - | 0.58 (0.07, 4.94) | |
| Foot pump + AES | - | 0.69 (0.08, 5.68) | |
| LMWH (high dose; extended duration) | - | 0.25 (0.01, 2.65) | |
| Versus UFH (standard duration) | LMWH (standard dose) + AES | - | 0.25 (0.08, 1.32) |
| LMWH (high dose; standard duration) | 0.66 (0.50, 0.87) | 0.48 (0.21, 0.94) | |
| IPCD | - | 1.30 (0.54, 3.17) | |
| LMWH (standard dose; extended duration) | - | 0.32 (0.10, 0.89) | |
| Dabigatran | - | 0.68 (0.20, 1.88) | |
| Foot pump | - | 1.03 (0.20, 3.55) | |
| Apixaban | - | 0.28 (0.05, 1.25) | |
| Rivaroxaban | - | 0.11 (0.03, 0.45) | |
| VKA (standard duration) | - | 0.74 (0.20, 2.17) | |
| UFH (extended duration) | 0.57 (0.18, 1.81) | 1.53 (0.31, 5.36) | |
| Aspirin | 4.17 (0.88, 19.66)* | 0.90 (0.14, 3.17) | |
| LMWH (low dose) + AES | - | 0.22 (0.03, 1.88) | |
| LMWH (extended duration) + AES | - | 0.14 (0.02, 1.27) | |
| Fondaparinux + AES | - | 0.11 (0.01, 1.02) | |
| AES (length unspecified) | - | 0.51 (0.11, 3.17) | |
| LMWH (low dose; pre-op) | - | 0.32 (0.04, 1.76) | |
| LMWH (low dose; post-op) | - | 0.39 (0.03, 4.24) | |
| VKA (extended duration) | - | 0.27 (0.02, 1.93) | |
| AES (above-knee) | - | 0.39 (0.03, 4.24) | |
| LMWH (high dose) + AES | - | 0.17 (0.01, 2.17) | |
| UFH + AES | - | 0.45 (0.05, 3.89) | |
| Foot pump + AES | - | 0.53 (0.06, 4.48) | |
| LMWH (high dose; extended duration) | - | 0.20 (0.01, 2.16) | |
| Versus LMWH (standard dose) + AES | LMWH (high dose; standard duration) | - | 1.82 (0.28, 8.24) |
| IPCD | - | 5.36 (0.99, 13.82) | |
| LMWH (standard dose; extended duration) | - | 1.21 (0.17, 6.59) | |
| Dabigatran | - | 2.61 (0.36, 10.81) | |
| Foot pump | - | 4.10 (0.43, 14.18) | |
| Apixaban | - | 1.06 (0.10, 7.73) | |
| Rivaroxaban | - | 0.42 (0.05, 3.30) | |
| VKA (standard duration) | - | 2.85 (0.38, 11.60) | |
| UFH (extended duration) | - | 6.67 (0.60, 16.55) | |
| Aspirin | - | 3.54 (0.27, 14.52) | |
| LMWH (low dose) + AES | 0.77 (0.48, 1.24) | 0.84 (0.18, 3.53) | |
| LMWH (extended duration) + AES | 0.61 | 0.52 (0.10, 2.59) | |
| Fondaparinux + AES | 0.44 (0.30, 0.64)* | 0.43 (0.08, 2.03) | |
| AES (length unspecified) | 1.58 (1.22, 2.06)* | 2.00 (0.79, 4.61) | |
| LMWH (low dose; pre-op) | - | 1.19 (0.08, 9.72) | |
| LMWH (low dose; post-op) | - | 1.49 (0.11, 10.76) | |
| VKA (extended duration) | - | 1.00 (0.05, 10.12) | |
| AES (above-knee) | - | 1.51 (0.16, 8.73) | |
| LMWH (high dose) + AES | - | 0.63 (0.06, 4.95) | |
| UFH + AES | - | 1.74 (0.29, 7.26) | |
| Foot pump + AES | - | 2.07 (0.36, 8.34) | |
| LMWH (high dose; extended duration) | - | 0.74 (0.02, 10.73) | |
| Versus LMWH (high dose; standard duration) | IPCD | - | 2.76 (1.01, 8.59) |
| LMWH (standard dose; extended duration) | - | 0.68 (0.20, 2.20) | |
| Dabigatran | - | 1.41 (0.40, 4.90) | |
| Foot pump | - | 2.10 (0.41, 9.28) | |
| Apixaban | - | 0.60 (0.10, 3.03) | |
| Rivaroxaban | 0.24 (0.05, 1.03) | ||
| VKA (standard duration) | 1.35 (0.70, 2.61)* | 1.53 (0.40, 5.64) | |
| UFH (extended duration) | - | 3.18 (0.58, 15.07) | |
| Aspirin | - | 1.83 (0.28, 8.93) | |
| LMWH (low dose) + AES | - | 0.47 (0.05, 4.83) | |
| LMWH (extended duration) + AES | - | 0.29 (0.03, 3.28) | |
| Fondaparinux + AES | - | 0.24 (0.02, 2.66) | |
| AES (length unspecified) | - | 1.10 (0.18, 8.35) | |
| LMWH (low dose; pre-op) | - | 0.67 (0.08, 4.33) | |
| LMWH (low dose; post-op) | - | 0.83 (0.10, 5.05) | |
| VKA (extended duration) | - | 0.57 (0.04, 4.71) | |
| AES (above-knee) | - | 0.83 (0.05, 10.87) | |
| LMWH (high dose) + AES | - | 0.36 (0.02, 5.52) | |
| UFH + AES | - | 0.96 (0.09, 9.94) | |
| Foot pump + AES | - | 1.14 (0.11, 11.68) | |
| LMWH (high dose; extended duration) | - | 0.42 (0.02, 5.12) | |
| Versus IPCD | LMWH (standard dose; extended duration) | - | 0.25 (0.07, 0.79) |
| Dabigatran | - | 0.52 (0.14, 1.62) | |
| Foot pump | - | 0.79 (0.14, 2.94) | |
| Apixaban | - | 0.21 (0.03, 1.05) | |
| Rivaroxaban | 0.08 (0.02, 0.39) | ||
| VKA (standard duration) | 1.00 (0.47, 2.11)* | 0.56 (0.17, 1.48) | |
| UFH (extended duration) | - | 1.19 (0.19, 4.86) | |
| Aspirin | - | 0.69 (0.09, 3.01) | |
| LMWH (low dose) + AES | - | 0.17 (0.02, 1.43) | |
| LMWH (extended duration) + AES | - | 0.10 (0.01, 0.98) | |
| Fondaparinux + AES | - | 0.08 (0.01, 0.79) | |
| AES (length unspecified) | - | 0.38 (0.09, 2.44) | |
| LMWH (low dose; pre-op) | - | 0.24 (0.03, 1.27) | |
| LMWH (low dose; post-op) | - | 0.30 (0.04, 1.46) | |
| VKA (extended duration) | - | 0.20 (0.02, 1.39) | |
| AES (above-knee) | - | 0.30 (0.02, 3.21) | |
| LMWH (high dose) + AES | - | 0.13 (0.01, 1.65) | |
| UFH + AES | - | 0.34 (0.04, 2.95) | |
| Foot pump + AES | - | 0.40 (0.05, 3.44) | |
| LMWH (high dose; extended duration) | - | 0.15 (0.01, 1.55) | |
| Versus LMWH (standard dose; extended duration) | Dabigatran | - | 2.06 (0.56, 7.82) |
| Foot pump | - | 3.07 (0.59, 14.78) | |
| Apixaban | 0.87 (0.14, 4.73) | ||
| Rivaroxaban | 0.22 (0.12, 0.41)* | 0.35 (0.10, 1.18) | |
| VKA (standard duration) | - | 2.24 (0.55, 9.29) | |
| UFH (extended duration) | - | 4.68 (0.74, 26.51) | |
| Aspirin | - | 2.67 (0.35, 15.99) | |
| LMWH (low dose) + AES | - | 0.70 (0.07, 7.90) | |
| LMWH (extended duration) + AES | - | 0.43 (0.04, 5.27) | |
| Fondaparinux + AES | - | 0.36 (0.03, 4.31) | |
| AES (length unspecified) | - | 1.64 (0.24, 13.76) | |
| LMWH (low dose; pre-op) | - | 0.98 (0.11, 6.93) | |
| LMWH (low dose; post-op) | - | 1.21 (0.14, 8.14) | |
| VKA (extended duration) | - | 0.83 (0.06, 7.45) | |
| AES (above-knee) | - | 1.23 (0.07, 17.59) | |
| LMWH (high dose) + AES | - | 0.52 (0.03, 8.87) | |
| UFH + AES | - | 1.42 (0.12, 16.35) | |
| Foot pump + AES | - | 1.68 (0.15, 18.95) | |
| LMWH (high dose; extended duration) | - | 0.62 (0.03, 8.12) | |
| Versus Dabigatran | Foot pump | - | 1.49 (0.27, 7.25) |
| Apixaban | - | 0.42 (0.06, 2.34) | |
| Rivaroxaban | - | 0.17 (0.03, 0.82) | |
| VKA (standard duration) | - | 1.09 (0.25, 4.63) | |
| UFH (extended duration) | - | 2.24 (0.35, 13.01) | |
| Aspirin | - | 1.31 (0.16, 7.71) | |
| LMWH (low dose) + AES | - | 0.33 (0.04, 3.71) | |
| LMWH (extended duration) + AES | - | 0.21 (0.02, 2.50) | |
| Fondaparinux + AES | - | 0.17 (0.02, 2.00) | |
| AES (length unspecified) | - | 0.77 (0.14, 6.46) | |
| LMWH (low dose; pre-op) | - | 0.48 (0.05, 3.38) | |
| LMWH (low dose; post-op) | - | 0.59 (0.04, 8.23) | |
| VKA (extended duration) | - | 0.40 (0.03, 3.63) | |
| AES (above-knee) | - | 0.59 (0.04, 8.28) | |
| LMWH (high dose) + AES | - | 0.25 (0.02, 4.14) | |
| UFH + AES | - | 0.68 (0.07, 7.66) | |
| Foot pump + AES | - | 0.80 (0.08, 8.80) | |
| LMWH (high dose; extended duration) | - | 0.30 (0.01, 3.96) | |
| Versus Foot pump | Apixaban | - | 0.28 (0.04, 2.07) |
| Rivaroxaban | - | 0.11 (0.02, 0.74) | |
| VKA (standard duration) | - | 0.73 (0.14, 4.23) | |
| UFH (extended duration) | - | 1.49 (0.20, 11.19) | |
| Aspirin | - | 0.88 (0.10, 6.72) | |
| LMWH (low dose) + AES | - | 0.22 (0.03, 2.93) | |
| LMWH (extended duration) + AES | - | 0.14 (0.01, 1.97) | |
| Fondaparinux + AES | - | 0.11 (0.01, 1.58) | |
| AES (length unspecified) | - | 0.50 (0.10, 5.34) | |
| LMWH (low dose; pre-op) | - | 0.32 (0.03, 2.84) | |
| LMWH (low dose; post-op) | - | 0.40 (0.04, 3.41) | |
| VKA (extended duration) | - | 0.27 (0.02, 3.07) | |
| AES (above-knee) | - | 0.39 (0.03, 6.37) | |
| LMWH (high dose) + AES | - | 0.17 (0.01, 3.15) | |
| UFH + AES | - | 0.44 (0.05, 6.03) | |
| Foot pump + AES | - | 0.52 (0.06, 7.07) | |
| LMWH (high dose; extended duration) | - | 0.20 (0.01, 3.16) | |
| Versus Apixaban | Rivaroxaban | - | 0.40 (0.06, 3.02) |
| VKA (standard duration) | - | 2.57 (0.43, 17.96) | |
| UFH (extended duration) | - | 5.35 (0.64, 48.48) | |
| Aspirin | - | 3.04 (0.30, 28.57) | |
| LMWH (low dose) + AES | - | 0.80 (0.06, 12.74) | |
| LMWH (extended duration) + AES | - | 0.50 (0.04, 8.55) | |
| Fondaparinux + AES | - | 0.41 (0.03, 6.87) | |
| AES (length unspecified) | - | 1.88 (0.21, 23.11) | |
| LMWH (low dose; pre-op) | - | 1.13 (0.09, 11.98) | |
| LMWH (low dose; post-op) | - | 1.38 (0.12, 14.17) | |
| VKA (extended duration) | - | 0.95 (0.05, 12.43) | |
| AES (above-knee) | - | 1.41 (0.07, 28.04) | |
| LMWH (high dose) + AES | - | 0.61 (0.03, 13.84) | |
| UFH + AES | - | 1.63 (0.11, 26.26) | |
| Foot pump + AES | - | 1.92 (0.14, 30.62) | |
| LMWH (high dose; extended duration) | - | 0.71 (0.02, 12.98) | |
| Versus Rivaroxaban | VKA (standard duration) | - | 6.41 (1.23, 35.36) |
| UFH (extended duration) | - | 13.43 (1.70, 96.91) | |
| Aspirin | - | 7.61 (0.84, 58.00) | |
| LMWH (low dose) + AES | - | 2.01 (0.15, 27.57) | |
| LMWH (extended duration) + AES | - | 1.26 (0.09, 18.53) | |
| Fondaparinux + AES | - | 1.03 (0.07, 14.83) | |
| AES (length unspecified) | - | 4.78 (0.50, 49.19) | |
| LMWH (low dose; pre-op) | - | 2.79 (0.27, 24.81) | |
| LMWH (low dose; post-op) | - | 3.42 (0.34, 29.03) | |
| VKA (extended duration) | - | 2.35 (0.15, 26.30) | |
| AES (above-knee) | - | 3.55 (0.17, 60.68) | |
| LMWH (high dose) + AES | - | 1.52 (0.07, 30.36) | |
| UFH + AES | - | 4.11 (0.27, 56.89) | |
| Foot pump + AES | - | 4.83 (0.34, 66.14) | |
| LMWH (high dose; extended duration) | - | 1.75 (0.07, 27.90) | |
| Versus VKA (standard duration) | UFH (extended duration) | - | 2.06 (0.31, 12.35) |
| Aspirin | - | 1.20 (0.14, 7.43) | |
| LMWH (low dose) + AES | - | 0.30 (0.03, 3.47) | |
| LMWH (extended duration) + AES | - | 0.19 (0.02, 2.32) | |
| Fondaparinux + AES | - | 0.15 (0.02, 1.87) | |
| AES (length unspecified) | - | 0.71 (0.13, 6.14) | |
| LMWH (low dose; pre-op) | 0.45 (0.31, 0.64) | 0.44 (0.09, 1.64) | |
| LMWH (low dose; post-op) | 0.55 (0.39, 0.76) | 0.54 (0.11, 1.91) | |
| VKA (extended duration) | 0.36 (0.10, 1.33) | 0.37 (0.04, 1.94) | |
| AES (above-knee) | - | 0.54 (0.04, 7.78) | |
| LMWH (high dose) + AES | - | 0.23 (0.01, 3.87) | |
| UFH + AES | - | 0.62 (0.06, 7.21) | |
| Foot pump + AES | - | 0.74 (0.07, 8.33) | |
| LMWH (high dose; extended duration) | 0.74 (0.38, 1.44) | 0.28 (0.02, 2.29) | |
| Versus UFH (extended duration) | Aspirin | - | 0.59 (0.06, 4.37) |
| LMWH (low dose) + AES | - | 0.14 (0.02, 1.98) | |
| LMWH (extended duration) + AES | - | 0.09 (0.01, 1.33) | |
| Fondaparinux + AES | - | 0.07 (0.01, 1.09) | |
| AES (length unspecified) | - | 0.31 (0.07, 3.72) | |
| LMWH (low dose; pre-op) | - | 0.21 (0.02, 2.09) | |
| LMWH (low dose; post-op) | - | 0.26 (0.02, 2.48) | |
| VKA (extended duration) | - | 0.18 (0.01, 2.13) | |
| AES (above-knee) | - | 0.25 (0.02, 4.28) | |
| LMWH (high dose) + AES | 0.11 (0.01, 2.13) | ||
| UFH + AES | - | 0.29 (0.03, 4.15) | |
| Foot pump + AES | - | 0.34 (0.04, 4.88) | |
| LMWH (high dose; extended duration) | - | 0.13 (0.00, 2.17) | |
| Versus Aspirin | LMWH (low dose) + AES | - | 0.25 (0.03, 4.42) |
| LMWH (extended duration) + AES | - | 0.16 (0.01, 2.93) | |
| Fondaparinux + AES | - | 0.13 (0.01, 2.36) | |
| AES (length unspecified) | - | 0.57 (0.10, 8.17) | |
| LMWH (low dose; pre-op) | - | 0.37 (0.03, 4.39) | |
| LMWH (low dose; post-op) | - | 0.46 (0.04, 5.28) | |
| VKA (extended duration) | - | 0.31 (0.02, 4.50) | |
| AES (above-knee) | - | 0.45 (0.03, 9.51) | |
| LMWH (high dose) + AES | - | 0.19 (0.01, 4.71) | |
| UFH + AES | - | 0.51 (0.05, 9.06) | |
| Foot pump + AES | - | 0.60 (0.06, 10.77) | |
| LMWH (high dose; extended duration) | - | 0.23 (0.01, 4.53) | |
| Versus LMWH (low dose) + AES | LMWH (extended duration) + AES | - | 0.62 (0.07, 5.81) |
| Fondaparinux + AES | - | 0.51 (0.06, 4.65) | |
| AES (length unspecified) | 1.61 (1.04, 2.52) | 2.35 (0.56, 10.69) | |
| LMWH (low dose; pre-op) | - | 1.41 (0.07, 19.95) | |
| LMWH (low dose; post-op) | - | 1.75 (0.09, 22.86) | |
| VKA (extended duration) | - | 1.18 (0.04, 19.61) | |
| AES (above-knee) | 1.45 (1.00, 2.11) | 1.75 (0.35, 7.07) | |
| LMWH (high dose) + AES | - | 0.75 (0.05, 9.99) | |
| UFH + AES | - | 2.04 (0.26, 14.28) | |
| Foot pump + AES | - | 2.40 (0.32, 16.79) | |
| LMWH (high dose; extended duration) | - | 0.87 (0.02, 19.76) | |
| Versus LMWH (standard dose; extended duration) + AES | Fondaparinux + AES | - | 0.81 (0.08, 8.23) |
| AES (length unspecified) | - | 3.80 (0.60, 25.16) | |
| LMWH (low dose; pre-op) | - | 2.25 (0.11, 35.36) | |
| LMWH (low dose; post-op) | - | 2.78 (0.13, 40.08) | |
| VKA (extended duration) | - | 1.89 (0.06, 35.03) | |
| AES (above-knee) | - | 2.84 (0.18, 33.96) | |
| LMWH (high dose) + AES | - | 1.20 (0.07, 17.55) | |
| UFH + AES | - | 3.28 (0.30, 30.52) | |
| Foot pump + AES | - | 3.88 (0.37, 35.78) | |
| LMWH (high dose; extended duration) | - | 1.39 (0.03, 35.31) | |
| Versus fondaparinux + AES | AES (length unspecified) | - | 4.65 (0.76, 29.22) |
| LMWH (low dose; pre-op) | - | 2.76 (0.13, 41.55) | |
| LMWH (low dose; post-op) | - | 3.41 (0.16, 47.41) | |
| VKA (extended duration) | - | 2.30 (0.08, 41.24) | |
| AES (above-knee) | - | 3.46 (0.22, 39.92) | |
| LMWH (high dose) + AES | 1.46 (1.01, 2.11) | 1.47 (0.29, 6.50) | |
| UFH + AES | - | 4.04 (0.38, 35.80) | |
| Foot pump + AES | - | 4.75 (0.47, 41.79) | |
| LMWH (high dose; extended duration) | - | 1.70 (0.04, 41.28) | |
| Versus AES (length unspecified) | LMWH (low dose; pre-op) | - | 0.60 (0.04, 6.00) |
| LMWH (low dose; post-op) | - | 0.74 (0.05, 6.71) | |
| VKA (extended duration) | - | 0.50 (0.02, 6.09) | |
| AES (above-knee) | - | 0.76 (0.08, 4.60) | |
| LMWH (high dose) + AES | - | 0.32 (0.03, 3.00) | |
| UFH + AES | 1.46 (1.01, 2.11) | 0.87 (0.20, 3.00) | |
| Foot pump + AES | 0.26 (0.09, 0.70) | 1.03 (0.24, 3.48) | |
| LMWH (high dose; extended duration) | - | 0.37 (0.01, 6.24) | |
| Versus LMWH (low dose; standard duration; pre-op) | LMWH (low dose; post-op) | 1.23 (0.81, 1.85)* | 1.22 (0.28, 5.44) |
| VKA (extended duration) | - | 0.85 (0.07, 8.65) | |
| AES (above-knee) | - | 1.25 (0.06, 31.23) | |
| LMWH (high dose) + AES | - | 0.54 (0.02, 15.05) | |
| UFH + AES | - | 1.45 (0.09, 29.53) | |
| Foot pump + AES | - | 1.70 (0.11, 34.69) | |
| LMWH (high dose; extended duration) | - | 0.64 (0.03, 9.39) | |
| Versus LMWH (low dose; standard duration; post-op) | VKA (extended duration) | - | 0.70 (0.06, 6.90) |
| AES (above-knee) | - | 1.01 (0.05, 24.79) | |
| LMWH (high dose) + AES | - | 0.44 (0.02, 11.93) | |
| UFH + AES | - | 1.17 (0.08, 23.26) | |
| Foot pump + AES | - | 1.38 (0.10, 27.44) | |
| LMWH (high dose; extended duration) | - | 0.52 (0.02, 7.44) | |
| Versus VKA (extended duration) | AES (above-knee) | - | 1.48 (0.06, 50.45) |
| LMWH (high dose) + AES | - | 0.65 (0.02, 24.76) | |
| UFH + AES | - | 1.73 (0.09, 49.88) | |
| Foot pump + AES | - | 2.03 (0.11, 58.64) | |
| LMWH (high dose; extended duration) | 0.74 (0.38, 1.44) | 0.76 (0.14, 3.29) | |
| Versus AES (above-knee) | LMWH (high dose) + AES | - | 0.43 (0.02, 8.95) |
| UFH + AES | - | 1.15 (0.11, 14.62) | |
| Foot pump + AES | - | 1.36 (0.13, 17.26) | |
| LMWH (high dose; extended duration) | - | 0.50 (0.01, 17.17) | |
| Versus LMWH (high dose + AES) | UFH + AES | - | 2.72 (0.18, 40.86) |
| Foot pump + AES | - | 3.20 (0.22, 48.42) | |
| LMWH (high dose; extended duration) | - | 1.16 (0.02, 42.98) | |
| Versus UFH + AES | Foot pump + AES | 0.38 (0.19, 0.76) | 1.18 (0.32, 4.50) |
| LMWH (high dose; extended duration) | - | 0.43 (0.01, 11.02) | |
| Versus Foot pump + AES | LMWH (high dose; extended duration) | - | 0.37 (0.01, 8.98) |
- *
Intervention and comparison numbers have been switched in Review Manager
Figure 828 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 26 different interventions being evaluated.

Figure 828Rank order for interventions based on the relative risk of experiencing DVT
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 570 compared with 634 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 90 reported. This corresponds well to the total number of trial arms, 88. The between trial standard deviation in the random effects analysis was 0.78 (95% CI 0.52 to 1.16). On evaluating inconsistency by comparing risk ratios, eight inconsistencies were identified. The NMA estimated risk ratio for:
- LMWH at a standard dose for a standard duration plus AES versus no prophylaxis (0.14 [0.07, 0.59]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.27 [0.15, 0.50])
- IPCD versus no prophylaxis (0.80 [0.34, 1.41]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.53 [0.40, 0.69])
- VKA at a standard duration versus LMWH at a standard dose and standard duration (0.94 [0.29, 2.52]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.57 [0.37, 0.86])
- LMWH at a high dose and standard duration versus UFH (0.48 [0.21, 0.94]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.66 [0.50, 0.87])
- LMWH at a high dose and extended duration versus VKA at a standard duration (0.28 [0.02, 2.29]) lay outside of the confidence interval of the risk ration estimated for the direct comparison (0.74 [0.38, 1.44])
- Foot pump plus AES (length unspecified) versus AES (length unspecified) (1.03 [0.24, 3.48]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.26 [0.09, 0.70])
- UFH plus AES (length unspecified) versus AES (length unspecified) (0.87 [0.20, 3.00]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (1.46 [1.01, 2.11])
- Foot pump plus AES (length unspecified) versus UFH plus AES (length unspecified) (1.18 [0.32, 4.50]) lay outside of the confidence interval of the risk ration estimated for the direct comparison (0.38 [0.19, 0.76])
An inconsistency model was run and the DIC statistics were as follows in Table 240. The difference in the DIC is small (<3–5) with the consistency model having the lower DIC value. This suggests that it fits the data better than the inconsistency model.
Table 240Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – DVT
| DIC | ResDev | |
|---|---|---|
| Consistency model | 570.092 | 90 |
| Inconsistency model | 570.268 | 90 |
M.1.3.2. Pulmonary embolism
Included studies
37 studies were identified as reporting on PE outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 30 studies involving 23 treatments were included in the network for PE. The network can be seen in Figure 829 and the trial data for each of the studies included in the NMA are presented in Table 241.

Figure 829Network diagram for PE
Table 241Study data for PE network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Comparison | Intervention 1 | Intervention 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | ||||
| Kalodiki 1996472 | No prophylaxis | LMWH (standard dose; standard duration) | LMWH (standard dose) + AES | 5 | 14 | 3 | 32 | 2 | 32 |
| Bergqvist 199692 | No prophylaxis | LMWH (standard dose; standard duration) | - | 2 | 116 | 0 | 117 | - | - |
| Torholm 1991941 | No prophylaxis | LMWH (standard dose; standard duration) | - | 1 | 54 | 0 | 58 | - | - |
| Hull 1990441 | No prophylaxis | IPCD (length unspecified) | - | 1 | 158 | 1 | 152 | - | - |
| Hardwick 2011389 | LMWH (standard dose; standard duration) | IPCD (length unspecified) | - | 2 | 196 | 2 | 194 | - | - |
| Avikainen 199557 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 0 | 84 | 1 | 83 | - | - |
| Colwell 1994204 | LMWH (standard dose; standard duration) | UFH (standard duration) | LMWH (high dose; standard duration) | 1 | 203 | 4 | 209 | 0 | 195 |
| Eriksson 1991A289 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 1 | 67 | 2 | 69 | - | - |
| Planès 1990758 | LMWH (standard dose; standard duration) | UFH (standard duration) | - | 0 | 120 | 1 | 106 | - | - |
| Comp 2001208 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 1 | 211 | 0 | 224 | - | - |
| Eriksson 2011292 | LMWH (standard dose; standard duration) | Dabigatran | - | 2 | 992 | 1 | 1001 | - | - |
| Eriksson 2007288 | LMWH (standard dose; standard duration) | Dabigatran | - | 3 | 897 | 5 | 880 | - | - |
| Warwick 1998994 | LMWH (standard dose; standard duration) | Foot pump | - | 0 | 138 | 1 | 136 | - | - |
| Lassen 2010534 | LMWH (standard dose; standard duration) | Apixaban | - | 5 | 2699 | 3 | 2708 | - | - |
| Kakkar 2008467 | LMWH (standard dose; standard duration) | Rivaroxaban | - | 4 | 869 | 1 | 864 | - | - |
| Dahl 1997227 | LMWH (standard dose) + AES | LMWH (extended duration) + AES | - | 3 | 106 | 0 | 111 | - | - |
| Lassen 2002526 | LMWH (standard dose) + AES | Fondaparinux + AES | - | 3 | 1123 | 3 | 1129 | - | - |
| Fuji 2008A328 | LMWH (standard dose) + AES | LMWH (low dose) + AES | AES (length unspecified) | 1 | 80 | 0 | 81 | 0 | 86 |
| Warwick 1995A992 | LMWH (standard dose) + AES | AES (length unspecified) | - | 1 | 78 | 2 | 78 | - | - |
| Kakkar 2000468 | LMWH (high dose; standard duration) | UFH (standard duration) | - | 1 | 125 | 2 | 134 | - | - |
| Levine 1991551 | LMWH (high dose; standard duration) | UFH (standard duration) | - | 1 | 332 | 1 | 333 | - | - |
| Colwell 1999203 | LMWH (high dose; standard duration) | VKA (standard duration) | - | 6 | 1516 | 9 | 1495 | - | - |
| Samama 2002845 | LMWH (high dose; extended duration) | VKA (extended duration) | - | 0 | 643 | 4 | 636 | - | - |
| Zanasi 19881039 | UFH (standard duration) | Aspirin (standard duration) | - | 1 | 25 | 1 | 19 | - | - |
| Eriksson 2008291 | LMWH (standard dose; extended duration) | Rivaroxaban | - | 1 | 1558 | 4 | 1595 | - | - |
| Anderson 201340 | LMWH (standard dose; extended duration) | LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 3 | 398 | 0 | 380 | - | - |
| Turpie 2002K954 | Fondaparinux + AES | LMWH (high dose) + AES | - | 5 | 1126 | 0 | 1128 | - | - |
| Moskovtiz 1978657 | AES (length unspecified) | UFH + AES | - | 1 | 32 | 3 | 35 | - | - |
| Lassen 1991529 | LMWH (low dose) + AES | AES (above-knee) | - | 2 | 93 | 1 | 97 | - | - |
| Prandoni 2002771 | VKA (standard duration) | VKA (extended duration) | - | 1 | 176 | 0 | 184 | - | - |
N; number of events, NA; number analysed
NMA results
Table 242 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 242Risk ratios for PE
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no prophylaxis | LMWH (standard dose; standard duration) | 0.15 (0.04, 0.58) | 0.25 (0.06, 0.89) |
| LMWH (standard dose) + AES | 0.17 (0.04, 0.80) | 0.12 (0.02, 0.82) | |
| IPCD (length unspecified) | 1.04 (0.07, 16.47) | 0.41 (0.05, 2.97) | |
| UFH (standard duration) | - | 0.65 (0.10, 4.02) | |
| Rivaroxaban | - | 0.07 (0.00, 0.78) | |
| LMWH (standard dose; extended duration) | - | 0.02 (0.00, 0.34) | |
| LMWH (high dose; standard duration) | - | 0.21 (0.02, 2.09) | |
| Dabigatran | - | 0.29 (0.04, 1.87) | |
| Foot pump | - | 1.18 (0.03, 29.88) | |
| Apixaban | - | 0.14 (0.01, 1.21) | |
| AES (length unspecified) | - | 0.12 (0.01, 2.08) | |
| LMWH (low dose) + AES | - | 0.03 (0.00, 1.87) | |
| Fondaparinux + AES | - | 0.12 (0.01, 1.95) | |
| LMWH (extended duration) + AES | - | 0.01 (0.00, 0.31) | |
| Aspirin (standard duration) | - | 3.43 (0.09, 45.71) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.10) | |
| VKA (standard duration) | - | 0.33 (0.02, 4.32) | |
| UFH + AES | - | 0.45 (0.01, 18.78) | |
| AES (above-knee) | - | 0.17 (0.00, 24.69) | |
| LMWH (high dose) + AES | - | 0.00 (0.00, 0.30) | |
| VKA (extended duration) | 0.06 (0.00, 4.46) | ||
| LMWH (high dose; extended duration) | 0.00 (0.00, 0.81) | ||
| Versus LMWH (standard dose; standard duration) | LMWH (standard dose) + AES | 0.67 (0.12, 3.73) | 0.52 (0.05, 3.82) |
| IPCD (length unspecified) | 1.01 (0.14, 7.10)* | 1.63 (0.23, 11.08) | |
| UFH (standard duration) | 3.01 (0.82, 11.03)* | 2.60 (0.73, 10.33) | |
| Rivaroxaban | 0.25 (0.03, 2.25)* | 0.29 (0.02, 2.14) | |
| LMWH (standard dose; extended duration) | 0.30 (0.01, 7.37) | 0.08 (0.00, 1.00) | |
| LMWH (high dose; standard duration) | 0.35 (0.01, 8.47) | 0.87 (0.11, 5.55) | |
| Dabigatran | 1.21 (0.37, 3.96)* | 1.19 (0.27, 4.76) | |
| Foot pump | - | 4.51 (0.15, 118.90) | |
| Apixaban | 0.60 (0.14, 2.50)* | 0.57 (0.08, 3.18) | |
| AES (length unspecified) | - | 0.49 (0.02, 9.58) | |
| LMWH (low dose) + AES | - | 0.14 (0.00, 8.53) | |
| Fondaparinux + AES | 0.25 (0.03, 2.25)* | 0.51 (0.03, 8.51) | |
| LMWH (extended duration) + AES | - | 0.03 (0.00, 1.41) | |
| Aspirin (standard duration) | - | 13.34 (0.44, 181.20) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.33) | |
| VKA (standard duration) | - | 1.34 (0.11, 12.45) | |
| UFH + AES | - | 1.88 (0.03, 83.70) | |
| AES (above-knee) | - | 0.69 (0.00, 109.60) | |
| LMWH (high dose) + AES | - | 0.02 (0.00, 1.26) | |
| VKA (extended duration) | - | 0.25 (0.00, 14.26) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 2.76) | |
| Versus LMWH (standard dose; standard duration) + AES | IPCD (length unspecified) | - | 3.22 (0.22, 45.98) |
| UFH (standard duration) | - | 5.30 (0.48, 54.12) | |
| Rivaroxaban | - | 0.53 (0.02, 11.48) | |
| LMWH (standard dose; extended duration) | - | 0.15 (0.00, 4.70) | |
| LMWH (high dose; standard duration) | 0.97 (0.17, 5.47)* | 1.71 (0.09, 28.52) | |
| Dabigatran | - | 2.32 (0.19, 29.85) | |
| Foot pump | - | 10.44 (0.16, 143.60) | |
| Apixaban | - | 1.10 (0.07, 18.05) | |
| AES (length unspecified) | 0.97 (0.17, 21.61)* | 0.97 (0.11, 8.04) | |
| LMWH (low dose) + AES | 0.33 (0.01, 7.96) | 0.29 (0.00, 9.28) | |
| Fondaparinux + AES | - | 1.00 (0.13, 7.52) | |
| LMWH (extended duration) + AES | - | 0.07 (0.00, 1.37) | |
| Aspirin (standard duration) | - | 34.54 (0.52, 148.70) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.01 (0.00, 1.13) | |
| VKA (standard duration) | - | 2.66 (0.10, 50.54) | |
| UFH + AES | - | 3.64 (0.13, 90.72) | |
| AES (above-knee) | - | 1.38 (0.00, 128.90) | |
| LMWH (high dose) + AES | - | 0.04 (0.00, 1.49) | |
| VKA (extended duration) | - | 0.47 (0.00, 48.12) | |
| LMWH (high dose; extended duration) | - | 0.02 (0.00, 8.29) | |
| Versus IPCD | UFH (standard duration) | - | 1.61 (0.16, 16.85) |
| Rivaroxaban | - | 0.17 (0.01, 2.96) | |
| LMWH (standard dose; extended duration) | - | 0.05 (0.00, 1.21) | |
| LMWH (high dose; standard duration) | - | 0.54 (0.03, 7.90) | |
| Dabigatran | - | 0.73 (0.06, 7.96) | |
| Foot pump | - | 2.88 (0.05, 123.10) | |
| Apixaban | - | 0.35 (0.02, 4.70) | |
| AES (length unspecified) | - | 0.30 (0.01, 9.30) | |
| LMWH (low dose) + AES | - | 0.08 (0.00, 7.49) | |
| Fondaparinux + AES | - | 0.31 (0.01, 8.70) | |
| LMWH (extended duration) + AES | - | 0.02 (0.00, 1.30) | |
| Aspirin (standard duration) | - | 8.03 (0.16, 206.90) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.31) | |
| VKA (standard duration) | - | 0.83 (0.04, 15.75) | |
| UFH + AES | - | 1.16 (0.02, 74.21) | |
| AES (above-knee) | - | 0.42 (0.00, 96.92) | |
| LMWH (high dose) + AES | - | 0.01 (0.00, 1.17) | |
| VKA (extended duration) | - | 0.15 (0.00, 14.26) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 2.22) | |
| Versus UFH (standard duration) | Rivaroxaban | - | 0.11 (0.01, 1.19) |
| LMWH (standard dose; extended duration) | - | 0.03 (0.00, 0.52) | |
| LMWH (high dose; standard duration) | 0.35 (0.08, 1.47) | 0.34 (0.05, 1.40) | |
| Dabigatran | - | 0.45 (0.06, 2.97) | |
| Foot pump | - | 1.77 (0.04, 56.95) | |
| Apixaban | - | 0.21 (0.02, 1.85) | |
| AES (length unspecified) | - | 0.18 (0.01, 4.70) | |
| LMWH (low dose) + AES | - | 0.05 (0.00, 3.85) | |
| Fondaparinux + AES | - | 0.19 (0.01, 4.11) | |
| LMWH (extended duration) + AES | 0.01 (0.00, 0.65) | ||
| Aspirin (standard duration) | 2.88 (0.46, 18.06)* | 4.66 (0.21, 75.89) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.15) | |
| VKA (standard duration) | - | 0.52 (0.05, 3.60) | |
| UFH + AES | - | 0.70 (0.01, 39.25) | |
| AES (above-knee) | - | 0.26 (0.00, 48.78) | |
| LMWH (high dose) + AES | - | 0.01 (0.00, 0.57) | |
| VKA (extended duration) | 0.10 (0.00, 4.67) | ||
| LMWH (high dose; extended duration) | 0.00 (0.00, 0.92) | ||
| Versus Rivaroxaban | LMWH (standard dose; extended duration) | 0.31 (0.05, 1.78) | 0.28 (0.02, 2.17) |
| LMWH (high dose; standard duration) | - | 3.06 (0.18, 75.17) | |
| Dabigatran | - | 4.20 (0.33, 82.88) | |
| Foot pump | - | 16.83 (0.30, 1021.00) | |
| Apixaban | - | 2.01 (0.12, 45.80) | |
| AES (length unspecified) | - | 1.81 (0.04, 86.58) | |
| LMWH (low dose) + AES | - | 0.50 (0.00, 64.91) | |
| Fondaparinux + AES | - | 1.88 (0.05, 79.40) | |
| LMWH (extended duration) + AES | - | 0.11 (0.00, 11.74) | |
| Aspirin (standard duration) | - | 47.43 (0.94, 1872.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.02 (0.00, 0.84) | |
| VKA (standard duration) | - | 4.77 (0.20, 143.70) | |
| UFH + AES | - | 6.97 (0.07, 664.60) | |
| AES (above-knee) | - | 2.56 (0.00, 697.00) | |
| LMWH (high dose) + AES | - | 0.07 (0.00, 9.59) | |
| VKA (extended duration) | - | 0.88 (0.00, 113.30) | |
| LMWH (high dose; extended duration) | - | 0.04 (0.00, 18.95) | |
| Versus LMWH (standard dose; extended duration) | LMWH (high dose; standard duration) | - | 11.42 (0.41, 493.60) |
| Dabigatran | - | 15.57 (0.77, 598.20) | |
| Foot pump | - | 64.15 (0.82, 6018.00) | |
| Apixaban | - | 7.48 (0.29, 311.80) | |
| AES (length unspecified) | - | 6.64 (0.12, 558.20) | |
| LMWH (low dose) + AES | - | 1.84 (0.00, 346.30) | |
| Fondaparinux + AES | 3.91 (0.44, 34.92)* | 6.99 (0.13, 512.20) | |
| LMWH (extended duration) + AES | - | 0.40 (0.00, 63.43) | |
| Aspirin (standard duration) | - | 175.90 (2.45, 12110.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | 0.15 (0.01, 2.89)* | 0.07 (0.00, 1.46) | |
| VKA (standard duration) | - | 17.66 (0.48, 931.10) | |
| UFH + AES | - | 25.95 (0.21, 4081.00) | |
| AES (above-knee) | - | 9.84 (0.01, 3985.00) | |
| LMWH (high dose) + AES | - | 0.27 (0.00, 54.28) | |
| VKA (extended duration) | 3.27 (0.00, 650.10) | ||
| LMWH (high dose; extended duration) | 0.13 (0.00, 96.85) | ||
| Versus LMWH (high dose; standard duration) | Dabigatran | - | 1.36 (0.13, 16.37) |
| Foot pump | - | 5.31 (0.10, 274.50) | |
| Apixaban | - | 0.65 (0.05, 9.72) | |
| AES (length unspecified) | - | 0.57 (0.02, 20.87) | |
| LMWH (low dose) + AES | - | 0.15 (0.00, 16.59) | |
| Fondaparinux + AES | - | 0.59 (0.02, 18.62) | |
| LMWH (extended duration) + AES | - | 0.04 (0.00, 2.89) | |
| Aspirin (standard duration) | - | 14.19 (0.47, 387.50) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.01 (0.00, 0.62) | |
| VKA (standard duration) | 0.66 (0.23, 1.84) | 1.53 (0.37, 6.16) | |
| UFH + AES | - | 2.22 (0.03, 162.40) | |
| AES (above-knee) | - | 0.78 (0.00, 205.60) | |
| LMWH (high dose) + AES | - | 0.02 (0.00, 2.37) | |
| VKA (extended duration) | - | 0.30 (0.00, 10.82) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 2.07) | |
| Versus Dabigatran | Foot pump | - | 3.85 (0.10, 142.40) |
| Apixaban | - | 0.48 (0.04, 4.69) | |
| AES (length unspecified) | - | 0.41 (0.02, 11.16) | |
| LMWH (low dose) + AES | - | 0.11 (0.00, 9.14) | |
| Fondaparinux + AES | - | 0.43 (0.02, 10.35) | |
| LMWH (extended duration) + AES | - | 0.03 (0.00, 1.57) | |
| Aspirin (standard duration) | - | 11.07 (0.29, 226.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.36) | |
| VKA (standard duration) | - | 1.13 (0.07, 16.88) | |
| UFH + AES | - | 1.60 (0.02, 92.90) | |
| AES (above-knee) | - | 0.58 (0.00, 114.40) | |
| LMWH (high dose) + AES | - | 0.02 (0.00, 1.42) | |
| VKA (extended duration) | - | 0.21 (0.00, 16.13) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 2.81) | |
| Versus Foot pump | Apixaban | - | 0.12 (0.00, 5.59) |
| AES (length unspecified) | - | 0.09 (0.00, 9.71) | |
| LMWH (low dose) + AES | - | 0.03 (0.00, 6.62) | |
| Fondaparinux + AES | - | 0.10 (0.00, 9.98) | |
| LMWH (extended duration) + AES | - | 0.01 (0.00, 1.18) | |
| Aspirin (standard duration) | - | 2.49 (0.03, 224.30) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.26) | |
| VKA (standard duration) | - | 0.29 (0.00, 17.57) | |
| UFH + AES | - | 0.38 (0.00, 69.71) | |
| AES (above-knee) | - | 0.14 (0.00, 78.93) | |
| LMWH (high dose) + AES | - | 0.00 (0.00, 1.08) | |
| VKA (extended duration) | - | 0.05 (0.00, 12.09) | |
| LMWH (high dose; extended duration) | - | 0.00 (0.00, 1.54) | |
| Versus Apixaban | AES (length unspecified) | - | 0.87 (0.03, 30.52) |
| LMWH (low dose) + AES | - | 0.24 (0.00, 23.71) | |
| Fondaparinux + AES | - | 0.90 (0.03, 27.94) | |
| LMWH (extended duration) + AES | - | 0.06 (0.00, 4.03) | |
| Aspirin (standard duration) | - | 22.98 (0.56, 601.70) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.01 (0.00, 0.89) | |
| VKA (standard duration) | - | 2.38 (0.12, 44.65) | |
| UFH + AES | - | 3.36 (0.04, 231.40) | |
| AES (above-knee) | - | 1.23 (0.00, 292.10) | |
| LMWH (high dose) + AES | - | 0.04 (0.00, 3.49) | |
| VKA (extended duration) | - | 0.43 (0.00, 37.71) | |
| LMWH (high dose; extended duration) | - | 0.02 (0.00, 6.53) | |
| Versus AES (length unspecified) | LMWH (low dose) + AES | - | 0.30 (0.00, 9.69) |
| Fondaparinux + AES | - | 1.02 (0.06, 19.24) | |
| LMWH (extended duration) + AES | - | 0.06 (0.00, 2.97) | |
| Aspirin (standard duration) | - | 31.53 (0.32, 593.60) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.01 (0.00, 1.87) | |
| VKA (standard duration) | - | 2.75 (0.06, 106.00) | |
| UFH + AES | 2.74 (0.30, 25.05) | 3.59 (0.30, 63.62) | |
| AES (above-knee) | - | 1.43 (0.00, 186.90) | |
| LMWH (high dose) + AES | - | 0.04 (0.00, 2.98) | |
| VKA (extended duration) | - | 0.47 (0.00, 76.14) | |
| LMWH (high dose; extended duration) | - | 0.02 (0.00, 11.98) | |
| Versus LMWH (low dose) + AES | Fondaparinux + AES | - | 3.57 (0.07, 1617.00) |
| LMWH (extended duration) + AES | - | 0.22 (0.00, 154.80) | |
| Aspirin (standard duration) | - | 105.40 (0.46, 51270.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.03 (0.00, 53.02) | |
| VKA (standard duration) | - | 10.18 (0.08, 5399.00) | |
| UFH + AES | - | 13.70 (0.16, 8649.00) | |
| AES (above-knee) | 1.00 (0.06, 15.76) | 4.55 (0.14, 390.60) | |
| LMWH (high dose) + AES | - | 0.14 (0.00, 130.20) | |
| VKA (extended duration) | 1.71 (0.00, 2387.00) | ||
| LMWH (high dose; extended duration) | 0.07 (0.00, 248.80) | ||
| Versus fondaparinux + AES | LMWH (extended duration) + AES | - | 0.06 (0.00, 2.67) |
| Aspirin (standard duration) | - | 30.57 (0.33, 561.70) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.01 (0.00, 1.73) | |
| VKA (standard duration) | - | 2.65 (0.06, 93.52) | |
| UFH + AES | - | 3.69 (0.08, 153.80) | |
| AES (above-knee) | 1.00 (0.06, 15.76) | 1.38 (0.00, 216.10) | |
| LMWH (high dose) + AES | 0.09 (0.01, 1.64) | 0.05 (0.00, 0.76) | |
| VKA (extended duration) | - | 0.46 (0.00, 70.47) | |
| LMWH (high dose; extended duration) | - | 0.02 (0.00, 11.65) | |
| Versus LMWH (standard dose; extended duration) + AES | Aspirin (standard duration) | - | 464.20 (2.80, 242800.00) |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.15 (0.00, 254.00) | |
| VKA (standard duration) | - | 43.65 (0.43, 30520.00) | |
| UFH + AES | - | 64.47 (0.55, 48030.00) | |
| AES (above-knee) | - | 26.19 (0.01, 37000.00) | |
| LMWH (high dose) + AES | - | 0.66 (0.00, 571.60) | |
| VKA (extended duration) | - | 8.20 (0.00, 13090.00) | |
| LMWH (high dose; extended duration) | - | 0.34 (0.00, 1307.00) | |
| Versus aspirin (standard duration) | LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.00 (0.00, 0.08) |
| LMWH (high dose) + AES | - | 0.11 (0.00, 4.01) | |
| UFH + AES | - | 0.13 (0.00, 20.61) | |
| AES (above-knee) | - | 0.05 (0.00, 24.21) | |
| VKA (standard duration) | - | 0.00 (0.00, 0.32) | |
| VKA (extended duration) | - | 0.02 (0.00, 2.85) | |
| LMWH (high dose; extended duration) | - | 0.00 (0.00, 0.44) | |
| Versus LMWH (standard dose; standard duration) + aspirin (extended duration) | LMWH (high dose) + AES | - | 291.70 (2.02, 392100.00) |
| UFH + AES | - | 437.20 (1.06, 869900.00) | |
| AES (above-knee) | - | 169.70 (0.05, 610700.00) | |
| VKA (standard duration) | - | 4.35 (0.00, 11340.00) | |
| VKA (extended duration) | - | 51.11 (0.02, 143200.00) | |
| LMWH (high dose; extended duration) | - | 2.14 (0.00, 12350.00) | |
| Versus LMWH (high dose) + AES | UFH + AES | - | 1.43 (0.02, 133.70) |
| AES (above-knee) | - | 0.51 (0.00, 161.90) | |
| VKA (standard duration) | - | 0.01 (0.00, 1.86) | |
| VKA (extended duration) | - | 0.20 (0.00, 5.27) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 1.07) | |
| Versus UFH + AES | AES (above-knee) | - | 0.39 (0.00, 99.84) |
| VKA (standard duration) | - | 0.01 (0.00, 1.58) | |
| VKA (extended duration) | - | 0.12 (0.00, 41.97) | |
| LMWH (high dose; extended duration) | - | 0.00 (0.00, 5.61) | |
| Versus AES (above-knee) | VKA (standard duration) | - | 0.03 (0.00, 57.82) |
| VKA (extended duration) | - | 0.33 (0.00, 1053.00) | |
| LMWH (high dose; extended duration) | - | 0.01 (0.00, 100.60) | |
| Versus VKA (standard duration) | VKA (extended duration) | 0.32 (0.01, 7.78) | 12.18 (0.01, 23630.00) |
| LMWH (high dose; extended duration) | 0.11 (0.01, 2.04) | 0.54 (0.00, 2480.00) | |
| Versus VKA (extended duration | LMWH (high dose; extended duration) | - | 0.06 (0.00, 0.99) |
- *
Intervention and comparison numbers have been switched in Review Manager
Figure 830 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 23 different interventions being evaluated.

Figure 830Rank order for interventions based on the relative risk of experiencing PE
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 255 compared with 276 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 61 reported. This corresponds well to the total number of trial arms, 62. The between trial standard deviation in the random effects analysis was 0.41 (95% CI 0.14 to 1.04). On evaluating inconsistency by comparing risk ratios, one inconsistency was identified. The NMA estimated risk ratio for VKA at an extended duration versus VKA at a standard duration (12.18 [1.01, 23630.00]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.32 [0.01, 7.78]). An inconsistency model was run and the DIC statistics were as follows in Table 243. The difference in the DIC is small (<3–5) with the consistency model having the lower DIC value. This suggests that it fits the data better than the inconsistency model.
Table 243Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – PE
| DIC | ResDev | |
|---|---|---|
| Consistency model | 255.025 | 61 |
| Inconsistency model | 258.386 | 63 |
M.1.3.3. Major bleeding
Included studies
28 studies were identified as reporting on major bleeding outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 24 studies involving 15 treatments were included in the network for PE. The network can be seen in Figure 831 and the trial data for each of the studies included in the NMA are presented in Table 244.

Figure 831Network diagram for major bleeding
Table 244Study data for major bleeding network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Comparison | Intervention 1 | Intervention 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | ||||
| Moskovitz 1978657 | No prophylaxis/mechanical | UFH (standard duration) | - | 3 | 35 | 0 | 32 | - | - |
| Turpie 1986952 | No prophylaxis/mechanical | LMWH (high dose; standard duration) | - | 1 | 50 | 2 | 50 | - | - |
| Fuji 2008A328 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | LMWH (low dose; post-op) | 0 | 101 | 2 | 102 | 1 | 100 |
| Hardwick 2011389 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | - | 0 | 198 | 11 | 194 | - | - |
| Samama 1997844 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | - | 1 | 75 | 1 | 78 | - | - |
| Fuji 2008325 | No prophylaxis/mechanical | Fondaparinux | - | 0 | 82 | 2 | 81 | - | - |
| Levine 1991551 | UFH (standard duration) | LMWH (high dose; standard duration) | - | 19 | 332 | 11 | 333 | - | - |
| Colwell 1994204 | UFH (standard duration) | LMWH (high dose; standard duration) | LMWH (standard dose; standard duration) | 13 | 209 | 8 | 195 | 3 | 203 |
| Eriksson 1991A289 | UFH (standard duration) | LMWH (standard dose; standard duration) | - | 5 | 69 | 1 | 67 | - | - |
| Plànes 1990758 | UFH (standard duration) | LMWH (standard dose; standard duration) | - | 0 | 106 | 2 | 120 | - | - |
| Turpie 2002K954 | LMWH (high dose; standard duration) | Fondaparinux | - | 11 | 1129 | 20 | 1128 | - | - |
| Colwell 1999203 | LMWH (high dose; standard duration) | VKA (standard duration) | - | 6 | 1516 | 4 | 1495 | - | - |
| Lassen 2002526 | LMWH (standard dose; standard duration) | Fondaparinux | - | 32 | 1133 | 47 | 1140 | - | - |
| Francis 1997315 | LMWH (standard dose; standard duration) | VKA (standard duration) | - | 6 | 271 | 4 | 279 | - | - |
| Eriksson 2011292 | LMWH (standard dose; standard duration) | Dabigatran | - | 9 | 1003 | 14 | 1010 | - | - |
| Eriksson 2007288 | LMWH (standard dose; standard duration) | Dabigatran | - | 18 | 1154 | 23 | 1146 | - | - |
| Lassen 2010534 | LMWH (standard dose; standard duration) | Apixaban | - | 18 | 2659 | 22 | 2673 | - | - |
| Kakkar 2008467 | LMWH (standard dose; standard duration) | Rivaroxaban | - | 19 | 1257 | 23 | 1252 | - | - |
| Lassen 1998527 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 1 | 141 | 0 | 140 | - | - |
| Hull 2000440 | LMWH (low dose; post-op) | VKA (standard duration) | LMWH (low dose; pre-op) | 32 | 487 | 22 | 489 | 44 | 496 |
| Prandoni 2002771 | VKA (standard duration) | VKA (extended duration) | - | 0 | 176 | 1 | 184 | - | - |
| Eriksson 2008291 | LMWH (standard dose; extended duration) | Rivaroxaban | - | 33 | 2225 | 40 | 2266 | - | - |
| Anderson 201340 | LMWH (standard dose; extended duration) | LMWH (st; st duration) + aspirin (extended) | - | 1 | 400 | 0 | 386 | - | - |
| Samama 2002845 | LMWH (high dose; extended duration) | VKA (extended duration) | - | 10 | 643 | 37 | 636 | - | - |
N; number of events, NA; number analysed
NMA results
Table 245 summarises the results of the conventional meta-analyses in terms of odd ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of odd ratios for every possible treatment comparison. Relative risks were not calculated for this outcome as data was only available for non-surgical site bleeding (intracranial haemorrhage + gastrointestinal bleeding) from the observational study used as the source of baseline risk.451
Table 245Odd ratios for major bleeding
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no prophylaxis/mechanical | UFH (standard duration) | 7.00 (0.35, 140.99) | 3.58 (0.89, 13.67) |
| LMWH (high dose; standard duration) | 0.49 (0.04, 5.58) | 2.47 (0.67, 9.56) | |
| LMWH (standard dose; standard duration) | 7.66 (1.76, 33.31) | 2.55 (0.82, 8.70) | |
| Fondaparinux | 5.19 (0.25, 109.77) | 4.28 (1.07, 18.66) | |
| LMWH (low dose; post-op) | 3.06 (0.12, 76.02) | 2.20 (0.35, 13.35) | |
| VKA (standard duration) | - | 1.54 (0.31, 7.94) | |
| Dabigatran | - | 3.63 (0.74, 18.48) | |
| Apixaban | - | 3.16 (0.47, 21.15) | |
| Rivaroxaban | - | 2.74 (0.42, 16.16) | |
| LMWH (standard dose; extended duration) | - | 1.99 (0.21, 14.60) | |
| LMWH (low dose; pre-op) | - | 3.13 (0.41, 23.59) | |
| VKA (extended duration) | - | 8.21 (0.13, 7883.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.37 (0.00, 26.96) | |
| LMWH (high dose; extended duration) | - | 2.06 (0.02, 2194.00) | |
| Versus UFH | LMWH (high dose; standard duration) | 0.60 (0.33, 1.06) | 0.69 (0.28, 2.01) |
| LMWH (standard dose; standard duration) | 0.34 (0.14, 0.84) | 0.71 (0.28, 2.13) | |
| Fondaparinux | - | 1.18 (0.36, 5.06) | |
| LMWH (low dose; post-op) | - | 0.61 (0.11, 3.68) | |
| VKA (standard duration) | - | 0.43 (0.10, 2.01) | |
| Dabigatran | - | 1.00 (0.25, 4.99) | |
| Apixaban | - | 0.87 (0.16, 5.91) | |
| Rivaroxaban | - | 0.76 (0.14, 4.22) | |
| LMWH (standard dose; extended duration) | - | 0.55 (0.07, 3.86) | |
| LMWH (low dose; pre-op) | - | 0.87 (0.13, 6.53) | |
| VKA (extended duration) | - | 2.29 (0.04, 2198.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.10 (0.00, 7.53) | |
| LMWH (high dose; extended duration) | - | 0.57 (0.01, 621.20) | |
| Versus LMWH (high dose; standard duration) | LMWH (standard dose; standard duration) | 0.35 (0.09, 1.34) | 1.04 (0.38, 2.83) |
| Fondaparinux | 1.83 (0.87, 3.85)* | 1.71 (0.58, 5.66) | |
| LMWH (low dose; post-op) | - | 0.89 (0.17, 4.54) | |
| VKA (standard duration) | 0.68 (0.19, 2.40) | 0.62 (0.16, 2.36) | |
| Dabigatran | - | 1.46 (0.34, 6.58) | |
| Apixaban | - | 1.27 (0.21, 7.77) | |
| Rivaroxaban | - | 1.11 (0.19, 5.73) | |
| LMWH (standard dose; extended duration) | - | 0.80 (0.09, 5.27) | |
| LMWH (low dose; pre-op) | - | 1.26 (0.20, 8.08) | |
| VKA (extended duration) | - | 3.28 (0.06, 2993.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.15 (0.00, 10.57) | |
| LMWH (high dose; extended duration) | - | 0.83 (0.01, 851.90) | |
| Versus LMWH (standard dose; standard duration) | Fondaparinux | 1.48 (0.94, 2.34)* | 1.66 (0.58, 5.15) |
| LMWH (low dose; post-op) | 0.51 (0.05, 5.66) | 0.86 (0.18, 3.95) | |
| VKA (standard duration) | 0.64 (0.18, 2.30)* | 0.60 (0.16, 2.14) | |
| Dabigatran | 1.38 (0.84, 2.28)* | 1.41 (0.48, 4.27) | |
| Apixaban | 1.22 (0.65, 2.26)* | 1.23 (0.27, 5.51) | |
| Rivaroxaban | 1.22 (0.65, 2.28)* | 1.07 (0.25, 3.97) | |
| LMWH (standard dose; extended duration) | 0.33 (0.01, 8.25) | 0.78 (0.11, 3.85) | |
| LMWH (low dose; pre-op) | - | 1.22 (0.20, 7.15) | |
| VKA (extended duration) | - | 3.14 (0.06, 2820.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.14 (0.00, 8.94) | |
| LMWH (high dose; extended duration) | - | 0.79 (0.01, 815.60) | |
| Versus Fondaparinux | LMWH (low dose; post-op) | - | 0.51 (0.08, 2.97) |
| VKA (standard duration) | - | 0.36 (0.07, 1.67) | |
| Dabigatran | - | 0.85 (0.18, 3.89) | |
| Apixaban | - | 0.74 (0.11, 4.58) | |
| Rivaroxaban | - | 0.64 (0.10, 3.42) | |
| LMWH (standard dose; extended duration) | - | 0.47 (0.05, 3.11) | |
| LMWH (low dose; pre-op) | - | 0.73 (0.09, 5.23) | |
| VKA (extended duration) | - | 1.90 (0.03, 1816.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.09 (0.00, 6.02) | |
| LMWH (high dose; extended duration) | - | 0.48 (0.01, 500.80) | |
| Versus LMWH (low dose; post-op) | VKA (standard duration) | - | 0.70 (0.20, 2.61) |
| Dabigatran | - | 1.66 (0.26, 11.40) | |
| Apixaban | - | 1.43 (0.17, 12.73) | |
| Rivaroxaban | - | 1.25 (0.15, 9.64) | |
| LMWH (standard dose; extended duration) | - | 0.90 (0.08, 8.49) | |
| LMWH (low dose; pre-op) | 1.38 (0.86, 2.22) | 1.42 (0.35, 5.91) | |
| VKA (extended duration) | - | 3.68 (0.07, 3220.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.17 (0.00, 14.06) | |
| LMWH (high dose; extended duration) | - | 0.93 (0.01, 927.10) | |
| Versus VKA (standard duration) | Dabigatran | - | 2.36 (0.45, 12.91) |
| Apixaban | - | 2.05 (0.29, 14.69) | |
| Rivaroxaban | - | 1.77 (0.26, 11.11) | |
| LMWH (standard dose; extended duration) | - | 1.29 (0.13, 10.07) | |
| LMWH (low dose; pre-op) | 2.07 (1.22, 3.50) | 2.03 (0.49, 8.27) | |
| VKA (extended duration) | 2.89 (0.12, 71.31) | 5.18 (0.12, 4147.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.24 (0.00, 18.31) | |
| LMWH (high dose; extended duration) | 0.26 (0.13, 0.52) | 1.30 (0.02, 1200.00) | |
| Versus Dabigatran | Apixaban | - | 0.87 (0.13, 5.46) |
| Rivaroxaban | - | 0.76 (0.12, 4.06) | |
| LMWH (standard dose; extended duration) | - | 0.55 (0.06, 3.69) | |
| LMWH (low dose; pre-op) | - | 0.86 (0.10, 6.78) | |
| VKA (extended duration) | - | 2.26 (0.04, 2161.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.10 (0.00, 7.14) | |
| LMWH (high dose; extended duration) | 0.57 (0.01, 607.50) | ||
| Versus Apixaban | Rivaroxaban | - | 0.88 (0.10, 6.31) |
| LMWH (standard dose; extended duration) | - | 0.63 (0.05, 5.52) | |
| LMWH (low dose; pre-op) | - | 0.99 (0.10, 9.99) | |
| VKA (extended duration) | - | 2.64 (0.04, 2645.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.12 (0.00, 9.43) | |
| LMWH (high dose; extended duration) | - | 0.66 (0.01, 737.70) | |
| Versus Rivaroxaban | LMWH (standard dose; extended duration) | 0.82 (0.51, 1.30) | 0.73 (0.18, 2.54) |
| LMWH (low dose; pre-op) | - | 1.14 (0.12, 11.40) | |
| VKA (extended duration) | - | 3.01 (0.05, 3189.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.14 (0.00, 7.28) | |
| LMWH (high dose; extended duration) | - | 0.76 (0.01, 905.60) | |
| Versus LMWH (standard dose; extended duration) | LMWH (low dose; pre-op) | - | 1.58 (0.15, 21.45) |
| VKA (extended duration) | - | 4.24 (0.06, 4892.00) | |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | 0.35 (0.01, 8.51)* | 0.20 (0.00, 8.19) | |
| LMWH (high dose; extended duration) | - | 1.06 (0.01, 1347.00) | |
| Versus LMWH (low dose; standard duration; preop) | VKA (extended duration) | - | 2.62 (0.05, 2269.00) |
| LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.12 (0.00, 10.62) | |
| LMWH (high dose; extended duration) | - | 0.66 (0.01, 652.50) | |
| Versus VKA (extended duration | LMWH (standard dose; standard duration) + aspirin (extended duration) | - | 0.04 (0.00, 15.62) |
| LMWH (high dose; extended duration) | - | 0.25 (0.05, 1.14) | |
| Versus LMWH (standard dose; standard duration) + aspirin (extended duration) | LMWH (high dose; extended duration) | - | 6.97 (0.01, 64290.00) |
- *
Intervention and comparison numbers have been switched in Review Manager
Figure 832 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 14 different interventions being evaluated.

Figure 832Rank order for interventions based on the relative risk of experiencing major bleeding
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 275 compared with 276 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 55 reported. This corresponds well to the total number of trial arms, 51. The between trial standard deviation in the random effects analysis was 0.56 (95% CI 0.19 to 1.27). On evaluating inconsistency by comparing odd ratios, one inconsistency was identified. The NMA estimated odd ratio for LMWH at a standard dose for an extended duration versus VKA at a standard duration (1.30 [0.02, 1200.00]) lay outside of the confidence interval of the odd ratio estimated for the direct comparison (0.26 [0.13, 0.52]). An inconsistency model was run and the DIC statistics were as follows in Table 246. The difference in the DIC is small (<3–5) which suggests that there is no obvious inconsistency in the network. The consistency model has a smaller DIC suggesting that it is a better fit to the data than the inconsistency model.
Table 246Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – major bleeding
| DIC | ResDev | |
|---|---|---|
| Consistency model | 275.34 | 55 |
| Inconsistency model | 277.695 | 55 |
M.1.4. Discussion
Based on the results of conventional meta-analyses of direct evidence, as has been previously presented in Chapter 26 and appendix H, deciding upon the most clinical and cost effective prophylaxis intervention in patients undergoing elective hip replacement surgery is challenging. In order to overcome the difficulty of interpreting the conclusions from numerous separate comparisons, network meta-analysis of the direct evidence was performed. The findings of the NMA were used to facilitate the committee in their decision-making when developing recommendations.
Our analyses were divided into three critical outcomes. 42 studies informed the DVT network where 26 different individual or combination treatments were evaluated including five mechanical interventions, fourteen pharmacological interventions, and six interventions that combined both mechanical and pharmacological prophylaxis. 30 studies informed the PE network of 23 different treatments, including four mechanical interventions, eleven pharmacological interventions, and six interventions that combined both mechanical and pharmacological prophylaxis. The major bleeding network included 24 studies evaluating 15 treatments, 14 of which were pharmacological as for this outcome any mechanical prophylaxis measures were combined with the no prophylaxis intervention as it is believed that mechanical prophylaxis has no associated bleeding risk.
In the DVT network, the top three interventions were rivaroxaban, fondaparinux plus AES and LMWH at a standard dose for an extended duration plus AES. The bottom three interventions were no prophylaxis, UFH at an extended duration and IPCD (length unspecified). Five of the six interventions that represented a combination of mechanical and pharmacological prophylaxis featured in the top ten best ranked treatments. The treatment believed to most represent standard practice, LMWH at a standard dose for a standard duration plus AES, ranked at 7. There was a lot of uncertainty about the estimates with the credible intervals for some of the interventions being very wide, some interventions’ ranks spanning across from 1 to 26.
In the PE network, the top intervention was the combination treatment of LMWH at a standard dose for a standard duration followed by aspirin at an extended duration. The second and third ranked treatments were LMWH at a high dose for an extended duration and LMWH at a high dose for a standard duration plus AES. The bottom three interventions were aspirin at a standard duration, foot pump and no prophylaxis. The intervention LMWH at a standard dose for a standard duration with AES was ranked eleventh. There was also considerable uncertainty in the PE network with wide credible intervals for a majority of the interventions, particularly for LMWH (high dose, standard duration) plus AES and LMWH (low dose, standard duration) plus AES with credible intervals spanning from 1 to 20.; and for AES (above-knee) and apixaban with credible intervals spanning from 2 to 23.
In the major bleeding network the highest ranked intervention was the combination treatment of LMWH at a standard dose for a standard duration followed by aspirin at an extended duration. This was followed by no prophylaxis and VKA at a standard duration.. The bottom three interventions were VKA at an extended duration, fondaparinux and dabigatran. There was a lot of uncertainty within the major bleeding network with very wide credible intervals for all of the interventions. These very wide credible intervals account for the unusual rank of no prophylaxis as the second best intervention in terms of major bleeding.
In summary, the three outcomes chosen for analyses were considered to be among the most critical for assessing clinical effectiveness of different VTE prophylaxis strategies. All three networks seemed to fit well, as demonstrated by DIC and residual deviance statistics. However due to the sparse nature of the networks, and low event rates, the credible intervals around the ranking of treatments in all three networks were wide suggesting considerable uncertainty about these results.
M.1.5. Conclusion
This analysis allowed us to combine findings from many different comparisons presented in the review even when direct comparative data was lacking.
The committee and orthopaedic subgroup noted the wide credible intervals particularly for the PE and major bleeding network meta-analyses. They both also noted that even with the high levels of uncertainty, interventions such as LMWH at a standard dose for a standard duration followed by aspirin for an extended duration and LMWH in combination with AES, present possible clinical effectiveness in terms of the outcomes of DVT (symptomatic and asymptomatic), PE and major bleeding.
For details of the rationale and discussion leading to recommendations, please refer to the section linking the evidence to the recommendations (section 26.6, chapter 26).
M.1.6. WinBUGS codes
M.1.6.1. WinBUGS code for number of patients with DVT (symptomatic and asymptomatic)
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[4] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 85642
a <- 4746
for (k in 1:3){ # treatments below 4
logit(v[k]) <- logit(v[4]) - lor[k,4] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 5:NT){ # treatments above 4
logit(v[k]) <- logit(v[4]) + lor[4,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[4] <- v[4]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NT=26, NS=42,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: general physical health indicators
m.tau= -1.26, sd.tau=1.25 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
13 14 12 32 8 32 NA NA NA NA 1 2 4 NA NA 3
43 116 21 117 NA NA NA NA NA NA 1 2 NA NA NA 2
19 54 9 58 NA NA NA NA NA NA 1 2 NA NA NA 2
28 52 22 48 NA NA NA NA NA NA 1 3 NA NA NA 2
36 75 14 68 NA NA NA NA NA NA 1 3 NA NA NA 2
20 39 4 37 NA NA NA NA NA NA 1 5 NA NA NA 2
36 152 77 158 NA NA NA NA NA NA 1 6 NA NA NA 2
25 47 15 43 NA NA NA NA NA NA 1 6 NA NA NA 2
28 136 21 142 8 136 NA NA NA NA 2 3 5 NA NA 3
1 79 4 79 NA NA NA NA NA NA 2 3 NA NA NA 2
19 63 25 59 NA NA NA NA NA NA 2 3 NA NA NA 2
15 120 27 106 NA NA NA NA NA NA 2 3 NA NA NA 2
12 150 5 78 NA NA NA NA NA NA 2 5 NA NA NA 2
8 190 8 196 NA NA NA NA NA NA 2 6 NA NA NA 2
39 138 15 152 NA NA NA NA NA NA 2 7 NA NA NA 2
12 102 5 113 NA NA NA NA NA NA 2 7 NA NA NA 2
17 88 6 85 NA NA NA NA NA NA 2 7 NA NA NA 2
67 783 60 791 NA NA NA NA NA NA 2 8 NA NA NA 2
57 897 45 880 NA NA NA NA NA NA 2 8 NA NA NA 2
18 138 24 136 NA NA NA NA NA NA 2 9 NA NA NA 2
68 1911 22 1944 NA NA NA NA NA NA 2 10 NA NA NA 2
71 869 14 864 NA NA NA NA NA NA 2 11 NA NA NA 2
49 190 28 192 NA NA NA NA NA NA 2 12 NA NA NA 2
24 116 9 101 NA NA NA NA NA NA 3 5 NA NA NA 2
61 263 50 258 NA NA NA NA NA NA 3 5 NA NA NA 2
4 33 6 28 NA NA NA NA NA NA 3 13 NA NA NA 2
10 25 7 19 NA NA NA NA NA NA 3 14 NA NA NA 2
27 80 21 81 36 86 NA NA NA NA 4 15 18 NA NA 3
33 104 22 114 NA NA NA NA NA NA 4 16 NA NA NA 2
83 918 36 908 NA NA NA NA NA NA 4 17 NA NA NA 2
11 78 28 75 NA NA NA NA NA NA 4 18 NA NA NA 2
22 78 33 78 NA NA NA NA NA NA 4 18 NA NA NA 2
11 66 12 72 NA NA NA NA NA NA 6 12 NA NA NA 2
53 1558 12 1595 NA NA NA NA NA NA 7 11 NA NA NA 2
81 338 36 337 44 336 NA NA NA NA 12 19 20 NA NA 3
8 176 3 184 NA NA NA NA NA NA 12 21 NA NA NA 2
29 93 44 97 NA NA NA NA NA NA 15 22 NA NA NA 2
44 784 65 796 NA NA NA NA NA NA 17 23 NA NA NA 2
19 28 8 32 NA NA NA NA NA NA 18 24 NA NA NA 2
4 39 16 40 NA NA NA NA NA NA 18 25 NA NA NA 2
20 636 15 643 NA NA NA NA NA NA 21 26 NA NA NA 2
23 65 9 67 NA NA NA NA NA NA 24 25 NA NA NA 2
END
INITS
list(
d=c(NA,0,0,0,0, 0,0,0,1,2, 3,4,2,4,2, 1,2,-1,-2,0, 2,3,1,4,0, -1), # one for each treatment,
sd.sq=1,
mu=c(-2,0,2,0,0, 0,3,0,1,0, 0,2,1,1, 3, 2,-2,0,2,0, 0,0,3,0,1, 0,0,2,1, 1, 3, 2,1,0,4, 1, 2,0,2,-3, 1,1) )
list(
d=c(NA,0,0,4,0, 0,3,0,0,3, 4,4,1,0,-1, -3,0,2,1,4, 2,1,2,2,1, 0), # one for each treatment,
sd.sq=0.1,
mu=c(0,0,-2,0,3, 0,0,2,0,0, 0,2,0,2,1, 4,0,0,-2,0, 3,0,0,2,0, 0,0,2,0,2, 1,4, 2,0, -3, 1,2,1,0,0, 1,1) )
list(
d=c(NA,0,1,1,0, 0,0,0,1,2, 3,4,2,1,0, 3,1,3,4,-2, 0,1,-3,4,2, 1), # one for each treatment,
sd.sq=2,
mu=c(0,0,3,0,0, 0,0,0,3,3, 0,0,4,2,1, 1,0,0,3,0, 0,0,0,0,3, 3,0,0,4,2, 1,1,1, 2,4, 0,-1,2,1,3, 2,1) )
M.1.6.2. WinBUGS code for inconsistency model for number of patients with DVT
VTE - inconsistency model - Elective hip DVT ============================== 42 studies 26 treatments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=26,ns=42, m.tau= -1.26, sd.tau=1.25) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 13 14 12 32 8 32 NA NA NA NA 1 2 4 NA NA 3 43 116 21 117 NA NA NA NA NA NA 1 2 NA NA NA 2 19 54 9 58 NA NA NA NA NA NA 1 2 NA NA NA 2 28 52 22 48 NA NA NA NA NA NA 1 3 NA NA NA 2 36 75 14 68 NA NA NA NA NA NA 1 3 NA NA NA 2 20 39 4 37 NA NA NA NA NA NA 1 5 NA NA NA 2 36 152 77 158 NA NA NA NA NA NA 1 6 NA NA NA 2 25 47 15 43 NA NA NA NA NA NA 1 6 NA NA NA 2 28 136 21 142 8 136 NA NA NA NA 2 3 5 NA NA 3 1 79 4 79 NA NA NA NA NA NA 2 3 NA NA NA 2 19 63 25 59 NA NA NA NA NA NA 2 3 NA NA NA 2 15 120 27 106 NA NA NA NA NA NA 2 3 NA NA NA 2 12 150 5 78 NA NA NA NA NA NA 2 5 NA NA NA 2 8 190 8 196 NA NA NA NA NA NA 2 6 NA NA NA 2 39 138 15 152 NA NA NA NA NA NA 2 7 NA NA NA 2 12 102 5 113 NA NA NA NA NA NA 2 7 NA NA NA 2 17 88 6 85 NA NA NA NA NA NA 2 7 NA NA NA 2 67 783 60 791 NA NA NA NA NA NA 2 8 NA NA NA 2 57 897 45 880 NA NA NA NA NA NA 2 8 NA NA NA 2 18 138 24 136 NA NA NA NA NA NA 2 9 NA NA NA 2 68 1911 22 1944 NA NA NA NA NA NA 2 10 NA NA NA 2 71 869 14 864 NA NA NA NA NA NA 2 11 NA NA NA 2 49 190 28 192 NA NA NA NA NA NA 2 12 NA NA NA 2 24 116 9 101 NA NA NA NA NA NA 3 5 NA NA NA 2 61 263 50 258 NA NA NA NA NA NA 3 5 NA NA NA 2 4 33 6 28 NA NA NA NA NA NA 3 13 NA NA NA 2 10 25 7 19 NA NA NA NA NA NA 3 14 NA NA NA 2 27 80 21 81 36 86 NA NA NA NA 4 15 18 NA NA 3 33 104 22 114 NA NA NA NA NA NA 4 16 NA NA NA 2 83 918 36 908 NA NA NA NA NA NA 4 17 NA NA NA 2 11 78 28 75 NA NA NA NA NA NA 4 18 NA NA NA 2 22 78 33 78 NA NA NA NA NA NA 4 18 NA NA NA 2 11 66 12 72 NA NA NA NA NA NA 6 12 NA NA NA 2 53 1558 12 1595 NA NA NA NA NA NA 7 11 NA NA NA 2 81 338 36 337 44 336 NA NA NA NA 12 19 20 NA NA 3 8 176 3 184 NA NA NA NA NA NA 12 21 NA NA NA 2 29 93 44 97 NA NA NA NA NA NA 15 22 NA NA NA 2 44 784 65 796 NA NA NA NA NA NA 17 23 NA NA NA 2 19 28 8 32 NA NA NA NA NA NA 18 24 NA NA NA 2 4 39 16 40 NA NA NA NA NA NA 18 25 NA NA NA 2 20 636 15 643 NA NA NA NA NA NA 21 26 NA NA NA 2 23 65 9 67 NA NA NA NA NA NA 24 25 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(-2,0,2,0,0, 0,3,0,1,0, 0,2,1,1, 3, 2,-2,0,2,0, 0,0,3,0,1, 0,0,2,1,1, 3, 2,1,0,4, 1, 2,0,2,0, 1,2), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA, NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0 ), .Dim = c(25,26)) ) # chain 2 list(sd.sq=1.5, mu=c(0,0,-2,0,3, 0,0,2,0,0, 0,2,0,2,1, 4,0,0,-2,0, 3,0,0,2,0, 0,0,2,0,2, 1,4,2,0,-3, 1,2,1,0, 2, 2,0), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA, NA,NA,5 ), .Dim = c(25,26)) ) # chain 3 list(sd.sq=3, mu=c(0,0,3,0,0, 0,0,0,3,3, 0,0,4,2,1,1,0,0,3,0,0, 0,0,0,3,3, 0,0,4,2,1,1, 1, 2,4, 0,-1,2,1,1, 0,-1), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3 ), .Dim = c(25,26)) )
M.1.6.3. WinBUGS code for number of patients with PE
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[3] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 85642
a <- 583
for (k in 1:2){ # treatments below 3
logit(v[k]) <- logit(v[3]) - lor[k,3] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 4:NT){ # treatments above 3
logit(v[k]) <- logit(v[3]) + lor[3,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[3] <- v[3]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 4.
list(NT=23, NS=30,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: general physical health indicators
m.tau= -1.26, sd.tau=1.25 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
5 14 3 32 2 32 NA NA NA NA 1 2 3 NA NA 3
2.5 117 0.5 118 NA NA NA NA NA NA 1 2 NA NA NA 2
1.5 55 0.5 59 NA NA NA NA NA NA 1 2 NA NA NA 2
1 158 1 152 NA NA NA NA NA NA 1 4 NA NA NA 2
2 196 2 194 NA NA NA NA NA NA 2 4 NA NA NA 2
1.5 204 4.5 210 0.5 196 NA NA NA NA 2 5 8 NA NA 3
0.5 85 1.5 84 NA NA NA NA NA NA 2 5 NA NA NA 2
1 67 2 69 NA NA NA NA NA NA 2 5 NA NA NA 2
0.5 121 1.5 107 NA NA NA NA NA NA 2 5 NA NA NA 2
4 869 1 864 NA NA NA NA NA NA 2 6 NA NA NA 2
1.5 212 0.5 225 NA NA NA NA NA NA 2 7 NA NA NA 2
2 992 1 1001 NA NA NA NA NA NA 2 9 NA NA NA 2
3 897 5 880 NA NA NA NA NA NA 2 9 NA NA NA 2
0.5 139 1.5 137 NA NA NA NA NA NA 2 10 NA NA NA 2
5 2699 3 2708 NA NA NA NA NA NA 2 11 NA NA NA 2
1.5 81 0.5 87 0.5 82 NA NA NA NA 3 12 13 NA NA 3
1 78 2 78 NA NA NA NA NA NA 3 12 NA NA NA 2
3 1123 3 1129 NA NA NA NA NA NA 3 14 NA NA NA 2
3.5 107 0.5 112 NA NA NA NA NA NA 3 15 NA NA NA 2
2 134 1 125 NA NA NA NA NA NA 5 8 NA NA NA 2
1 332 1 333 NA NA NA NA NA NA 5 8 NA NA NA 2
0.5 26 1.5 20 NA NA NA NA NA NA 5 16 NA NA NA 2
4 1595 1 1558 NA NA NA NA NA NA 6 7 NA NA NA 2
3.5 399 0.5 381 NA NA NA NA NA NA 7 17 NA NA NA 2
6 1516 9 1495 NA NA NA NA NA NA 8 18 NA NA NA 2
1 32 3 35 NA NA NA NA NA NA 12 19 NA NA NA 2
0.5 94 1.5 98 NA NA NA NA NA NA 13 20 NA NA NA 2
5.5 1127 0.5 1129 NA NA NA NA NA NA 14 21 NA NA NA 2
1.5 177 0.5 185 NA NA NA NA NA NA 18 22 NA NA NA 2
4.5 637 0.5 644 NA NA NA NA NA NA 22 23 NA NA NA 2
END
list(
d=c(NA,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0, 0), # one for each treatment,
sd.sq=1,
mu=c(0,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0, 0,0,0,0, 0,0,0,0,0, 0,0,0,0,0) )
list(
d=c(NA,0,0,0,0, 0,0,0,0,1, 0,0,0,0,-1, 0,0,0,0,1, 0,-1, 0), # one for each treatment,
sd.sq=0.1,
mu=c(-1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1, -1,-1,-1,-1, -1,-1,-1,-1,-1, -1,-1,-1,-1,-1) )
list(
d=c(NA,0,0,0,2, -2,0,0,0,1, 0,0,0,0,-1, 2,0,0,0,1, -2,-1, -1), # one for each treatment,
sd.sq=2,
mu=c(0,1,-1,0,2, 0,1,-1,-2,0, 1,2,0,2,0, 0, 2,1,0,-2, 0,2,1,-2,0, 2,1,1,0,0) )
M.1.6.4. WinBUGS code for inconsistency model for number of patients with PE
VTE - inconsistency model - Elective hip PE ============================== 30 studies 23 treatments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=23,ns=30, m.tau= -1.26, sd.tau=1.25) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 5 14 3 32 2 32 NA NA NA NA 1 2 3 NA NA 3 2.5 117 0.5 118 NA NA NA NA NA NA 1 2 NA NA NA 2 1.5 55 0.5 59 NA NA NA NA NA NA 1 2 NA NA NA 2 1 158 1 152 NA NA NA NA NA NA 1 4 NA NA NA 2 2 196 2 194 NA NA NA NA NA NA 2 4 NA NA NA 2 1.5 204 4.5 210 0.5 196 NA NA NA NA 2 5 8 NA NA 3 0.5 85 1.5 84 NA NA NA NA NA NA 2 5 NA NA NA 2 1 67 2 69 NA NA NA NA NA NA 2 5 NA NA NA 2 0.5 121 1.5 107 NA NA NA NA NA NA 2 5 NA NA NA 2 4 869 1 864 NA NA NA NA NA NA 2 6 NA NA NA 2 1.5 212 0.5 225 NA NA NA NA NA NA 2 7 NA NA NA 2 2 992 1 1001 NA NA NA NA NA NA 2 9 NA NA NA 2 3 897 5 880 NA NA NA NA NA NA 2 9 NA NA NA 2 0.5 139 1.5 137 NA NA NA NA NA NA 2 10 NA NA NA 2 5 2699 3 2708 NA NA NA NA NA NA 2 11 NA NA NA 2 1.5 81 0.5 87 0.5 82 NA NA NA NA 3 12 13 NA NA 3 1 78 2 78 NA NA NA NA NA NA 3 12 NA NA NA 2 3 1123 3 1129 NA NA NA NA NA NA 3 14 NA NA NA 2 3.5 107 0.5 112 NA NA NA NA NA NA 3 15 NA NA NA 2 2 134 1 125 NA NA NA NA NA NA 5 8 NA NA NA 2 1 332 1 333 NA NA NA NA NA NA 5 8 NA NA NA 2 0.5 26 1.5 20 NA NA NA NA NA NA 5 16 NA NA NA 2 4 1595 1 1558 NA NA NA NA NA NA 6 7 NA NA NA 2 3.5 399 0.5 381 NA NA NA NA NA NA 7 17 NA NA NA 2 6 1516 9 1495 NA NA NA NA NA NA 8 18 NA NA NA 2 1 32 3 35 NA NA NA NA NA NA 12 19 NA NA NA 2 0.5 94 1.5 98 NA NA NA NA NA NA 13 20 NA NA NA 2 5.5 1127 0.5 1129 NA NA NA NA NA NA 14 21 NA NA NA 2 1.5 177 0.5 185 NA NA NA NA NA NA 18 22 NA NA NA 2 4.5 637 0.5 644 NA NA NA NA NA NA 22 23 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(0,0,3,0,0, 0,2,0,-1,0, 4,0,3,1,0, 0, 2,1,3,-2, 4,2,1,-3,0, 3,1,0,3,-2), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0 ), .Dim = c(22,23)) ) # chain 2 list(sd.sq=1.5, mu=c(0,2,1,0,-2, 0,3,0,4,0, 2,0,1,3,0, 0, 2,1,3,-2, 4,2,1,-3,0, 3,2,-1,0,0), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5 ), .Dim = c(22,23)) ) # chain 3 list(sd.sq=3, mu=c(0,3,3,0,4, 0,1,0,-2,0, 1,2,0,2,0, 0, 2,1,3,-2, 4,2,1,-3,0, 3,1,1,0,-1), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3 ), .Dim = c(22,23)) )
M.1.6.5. WinBUGS code for number of patients with major bleeding
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[4] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 85642
a <- 620
for (k in 1:3){ # treatments below 4
logit(v[k]) <- logit(v[4]) - lor[k,4] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 5:NT){ # treatments above 4
logit(v[k]) <- logit(v[4]) + lor[4,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[4] <- v[4]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NT=15, NS=24,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: adverse events
m.tau= -0.84, sd.tau=1.24 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
3.5 36 0.5 33 NA NA NA NA NA NA 1 2 NA NA NA 2
1 50 2 50 NA NA NA NA NA NA 1 3 NA NA NA 2
0.5 102 2.5 103 1.5 101 NA NA NA NA 1 4 6 NA NA 3
0.5 199 11.5 195 NA NA NA NA NA NA 1 4 NA NA NA 2
1 75 1 78 NA NA NA NA NA NA 1 4 NA NA NA 2
0.5 83 2.5 82 NA NA NA NA NA NA 1 5 NA NA NA 2
19 332 11 333 NA NA NA NA NA NA 2 3 NA NA NA 2
13 209 8 195 3 203 NA NA NA NA 2 3 4 NA NA 3
5 69 1 67 NA NA NA NA NA NA 2 4 NA NA NA 2
0.5 107 2.5 121 NA NA NA NA NA NA 2 4 NA NA NA 2
11 1129 20 1128 NA NA NA NA NA NA 3 5 NA NA NA 2
6 1516 4 1495 NA NA NA NA NA NA 3 7 NA NA NA 2
32 1133 47 1140 NA NA NA NA NA NA 4 5 NA NA NA 2
6 271 4 279 NA NA NA NA NA NA 4 7 NA NA NA 2
9 1003 14 1010 NA NA NA NA NA NA 4 8 NA NA NA 2
18 1154 23 1146 NA NA NA NA NA NA 4 8 NA NA NA 2
18 2659 22 2673 NA NA NA NA NA NA 4 9 NA NA NA 2
19 1257 23 1252 NA NA NA NA NA NA 4 10 NA NA NA 2
1.5 142 0.5 141 NA NA NA NA NA NA 4 11 NA NA NA 2
32 487 22 489 44 496 NA NA NA NA 6 7 12 NA NA 3
0.5 177 1.5 185 NA NA NA NA NA NA 7 13 NA NA NA 2
40 2266 33 2275 NA NA NA NA NA NA 10 11 NA NA NA 2
1.5 401 0.5 386 NA NA NA NA NA NA 11 14 NA NA NA 2
37 636 10 643 NA NA NA NA NA NA 13 15 NA NA NA 2
END
INITS
list(
d=c(NA,0,0,0,0, 0,0,0,1,2, 3,4,1,0,0), # one for each treatment
sd.sq=1,
mu=c(-2,0,2,0,0, 0,3,0,1,0, 0,2,1, 1, 3, 2,0, 0,1,2, 1,2,1,1) )
list(
d=c(NA,0,0,4,0, 0,3,0,0,3, 4,4,2,1,2), # one for each treatment
sd.sq=0.1,
mu=c(0,0,-2,0,3, 0,0,2,0,0, 0,2,0,2,1, 4,3,0,3,4, 1,0,-1,0) )
list(
d=c(NA,0,1,1,0, 0,0,0,1,2, 3,4,1,2,1), # one for each treatment
sd.sq=2,
mu=c(0,0,3,0,0, 0,0,0,3,3, 0,0,4,2,1, 1,-1,0,2,3, 2,-3,0,2) )
M.1.6.6. WinBUGS code for inconsistency model for number of patients with major bleeding
VTE - inconsistency model - Elective hip - major bleeding ============================== 24 studies 15 treatments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=15,ns=24, m.tau= -0.84, sd.tau=1.24) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 3.5 36 0.5 33 NA NA NA NA NA NA 1 2 NA NA NA 2 1 50 2 50 NA NA NA NA NA NA 1 3 NA NA NA 2 0.5 102 2.5 103 1.5 101 NA NA NA NA 1 4 6 NA NA 3 0.5 199 11.5 195 NA NA NA NA NA NA 1 4 NA NA NA 2 1 75 1 78 NA NA NA NA NA NA 1 4 NA NA NA 2 0.5 83 2.5 82 NA NA NA NA NA NA 1 5 NA NA NA 2 19 332 11 333 NA NA NA NA NA NA 2 3 NA NA NA 2 13 209 8 195 3 203 NA NA NA NA 2 3 4 NA NA 3 5 69 1 67 NA NA NA NA NA NA 2 4 NA NA NA 2 0.5 107 2.5 121 NA NA NA NA NA NA 2 4 NA NA NA 2 11 1129 20 1128 NA NA NA NA NA NA 3 5 NA NA NA 2 6 1516 4 1495 NA NA NA NA NA NA 3 7 NA NA NA 2 32 1133 47 1140 NA NA NA NA NA NA 4 5 NA NA NA 2 6 271 4 279 NA NA NA NA NA NA 4 7 NA NA NA 2 9 1003 14 1010 NA NA NA NA NA NA 4 8 NA NA NA 2 18 1154 23 1146 NA NA NA NA NA NA 4 8 NA NA NA 2 18 2659 22 2673 NA NA NA NA NA NA 4 9 NA NA NA 2 19 1257 23 1252 NA NA NA NA NA NA 4 10 NA NA NA 2 1.5 142 0.5 141 NA NA NA NA NA NA 4 11 NA NA NA 2 32 487 22 489 44 496 NA NA NA NA 6 7 12 NA NA 3 0.5 177 1.5 185 NA NA NA NA NA NA 7 13 NA NA NA 2 40 2266 33 2275 NA NA NA NA NA NA 10 11 NA NA NA 2 1.5 401 0.5 386 NA NA NA NA NA NA 11 14 NA NA NA 2 37 636 10 643 NA NA NA NA NA NA 13 15 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(-2,0,2,0,0, 0,3,0,1,0, 0,2,1,1,3, 2,-2,1,1,0, 0,0,0,0), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0), .Dim = c(14,15)) ) # chain 2 list(sd.sq=1.5, mu=c(0,0,-2,0,3, 0,0,2,0,0, 0,2,0,2,1, 4,0,2,-1,1, 0,1,0,0), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5 ), .Dim = c(14,15)) ) # chain 3 list(sd.sq=3, mu=c(0,0,3,0,0, 0,0,0,3,3, 0,0,4,2,1, 1,0,3,0,0, 2,1,0,0), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3), .Dim = c(14,15)) )
M.2. Network meta-analysis for elective knee replacement surgery
M.2.1. Introduction
The results of conventional meta-analyses of direct evidence alone (as presented in the GRADE profiles for Chapter 27 and forest plots in appendix L) does not help inform which intervention is most effective as VTE prophylaxis in patients undergoing elective knee replacement surgery. The challenge of interpretation has arisen for two reasons:
- In isolation, each pair-wise comparison does not inform the choice among the different treatments; in addition direct evidence is not available for some pair-wise comparisons in a randomised controlled trial.
- There are frequently multiple overlapping comparisons that could potentially give inconsistent estimates of effect.
To overcome these problems, a hierarchical Bayesian network meta-analysis (NMA) was performed. This type of analysis allows for the synthesis of data from direct and indirect comparisons without breaking randomisation and allows for the ranking of different interventions. In this case the outcomes were defined as:
- Deep vein thrombosis (DVT; symptomatic and asymptomatic)
- Major bleeding
The analysis also provided estimates of effect (with 95% credible intervals) for each intervention compared to one another and compared to a single baseline risk (in this case the baseline treatment was no prophylaxis or in the case of the major bleeding outcome a combination of no prophylaxis and mechanical prophylaxis). These estimates provide a useful clinical summary of the results and facilitate the formation of recommendations based on the best available evidence.
Conventional fixed effects meta-analysis assumes that the relative effect of one treatment compared to another is the same across an entire set of trials. In a random effects model, it is assumed that the relative effects are different in each trial but that they are from a single common distribution and that this distribution is common across all sets of trials.
Network meta-analysis requires an additional assumption over conventional meta-analysis. The additional assumption is that intervention A has the same effect on people in trials of intervention A compared to intervention B as it does for people in trials of intervention A versus intervention C, and so on. Thus, in a random effects network meta-analysis, the assumption is that intervention A has the same effect distribution across trials of A versus B, A versus C and so on.
This specific method is usually referred to as mixed-treatment comparisons analysis but we will continue to use the term network meta-analysis to refer generically to this kind of analysis. We do so since the term “network” better describes the data structure, whereas “mixed treatments” could easily be misinterpreted as referring to combinations of treatments.
M.2.2. Methods
M.2.2.1. Study selection
To estimate the relative risks, we performed an NMA that simultaneously used all the relevant RCT evidence from the clinical evidence review. As with conventional meta-analyses, this type of analysis does not break the randomisation of the evidence, nor does it make any assumptions about adding the effects of different interventions. The effectiveness of a particular treatment strategy combination will be derived only from randomised controlled trials that had that particular combination in a trial arm.
M.2.2.2. Outcome measures
The NMA evidence reviews for interventions considered three clinical efficacy outcomes identified from the clinical evidence review; number of people with DVT, number of people with PE and number of people with major bleeding. Other outcomes were not considered for the NMA as they were infrequently reported across the studies. The committee considered that these outcomes were the most critical clinical outcomes for testing effectiveness of VTE prophylaxis.
M.2.2.3. Comparability of interventions
The interventions compared in the model were those found in the randomised controlled trials and included in the clinical evidence review already presented in Chapter 27 of the full guideline and in appendix H. If an intervention was evaluated in a study that met the inclusion criteria for the network (that is if it reported at least one of the outcomes of interest and matched the inclusion criteria for the meta-analysis) then it was included in the network meta-analysis, otherwise it was excluded.
The treatments included in each network are shown in Table 247.
Table 247Treatments included in the network meta-analysis
|
Network 1: Number of people with DVT |
Network 2: Number of people with PE |
Network 3: Number of people with major bleeding |
|---|---|---|
| No prophylaxis | No prophylaxis | No prophylaxis/mechanical |
| LMWH (standard dose; standard duration) | LMWH (standard dose; standard duration) | LMWH (standard dose; standard duration) |
| LMWH (high dose; standard duration) | AES | LMWH (high dose; standard duration) |
| AES (length unspecified) | IPCD | Fondaparinux |
| Dabigatran | Dabigatran | LMWH (low dose; standard duration) |
| IPCD (length unspecified) | Rivaroxaban | Apixaban |
| Foot pump | Apixaban | Dabigatran |
| Foot pump + AES | LMWH (standard dose; extended duration) | Rivaroxaban |
| Rivaroxaban | LMWH (standard dose; standard duration) + AES | LMWH (standard dose; extended duration) |
| Aspirin | LMWH (low dose; standard duration) + AES | UFH |
| LMWH (standard duration; extended duration) | LMWH (high dose; standard duration) | VKA |
| Apixaban | VKA | - |
| VKA | UFH | - |
| UFH | - | - |
| Fondaparinux + AES | - | - |
| LMWH (standard dose; standard duration) + AES | - | - |
| LMWH (low dose; standard duration) + AES | - | - |
| LMWH high dose; standard duration) + AES | - | - |
| UFH + AES | - | - |
M.2.2.4. Baseline risks
The baseline risk is defined as the risk of achieving the outcome of interest in the baseline treatment arm of the included trials. This figure is useful because it allows us to convert the results of the NMA from odds ratios to relative risks. However, the majority of these trials were older studies that reported very high risk of DVT and PE in the no prophylaxis arm that the orthopaedic subgroup considered to be not reflective of the baseline risk in the UK. Hence, for the purpose of calculating the relative risks of these events for presentation in this appendix, the baseline risk values were obtained from data from the UK National Joint Registry (NJR).450 For full details of the calculation of baseline risk, please refer to HE write-up (appendix P, section P.1.3.3).
M.2.2.5. Statistical analysis
A hierarchical Bayesian network meta-analysis (NMA) was performed using the software WinBUGS. We adapted a three-arm random effects model template for the networks, from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). This model accounts for the correlation between study level effects induced by multi-arm trials.
In order to be included in the analysis, a fundamental requirement is that each treatment is connected directly or indirectly to every other intervention in the network. For each outcome subgroup, a diagram of the evidence network is presented in section M.2.3.
The model used was a random effects logistic regression model, with parameters estimated by Markov chain Monte Carlo simulation. As it was a Bayesian analysis, for each parameter the evidence distribution is weighted by a distribution of prior beliefs. Due to the sparse nature of the networks (few studies per direct treatment comparison), the between-study heterogeneity parameter is imprecisely estimated in a random effects model. Therefore it is beneficial to apply informative priors in order to restrict the prior distribution for heterogeneity to avoid unreasonably wide credible intervals. Turner et al (2015)946 derived a novel set of predictive distributions for the degree of heterogeneity across 80 different settings. Appropriate predictive distributions for heterogeneity were chosen from Turner et al (2015)946 and used directly as informative priors. The log normal (µ, ơ2) predictive distributions obtained for the between-study heterogeneity in a future meta-analysis presented in Table IV946 were selected according to the outcome and treatment comparison. For the DVT and PE NMAs the distributions defined by the outcome of “general physical health indicators” and by the intervention/comparison type “non-pharmacological vs. pharmacological” were chosen (LN[−1.26, 1.252]). For the major bleeding NMA the distributions defined by the outcome of “adverse events” and by the intervention/comparison type “non-pharmacological vs. pharmacological” were chosen (LN[−0.84, 1.242]). These distributions were chosen as they represented outcomes measured by an assessor, whose method of measurement as well as judgement may influence the outcome (as studies provided slightly variable ways of defining these critical outcomes), and the interaction aspect encompassed both the pharmacological and mechanical prophylaxis options covered in our review protocol.
For the analyses, a series of 60,000 burn-in simulations were run to allow convergence and then a further 60,000 simulations were run to produce the outputs. Convergence was assessed by examining the history and kernel density plots.
We tested the goodness of fit of the model by calculating the residual deviance. If the residual deviance is close to the number of unconstrained data points (the number of trial arms in the analysis) then the model is explaining the data well.
The results, in terms of relative risk, of pair-wise meta-analyses are presented in the clinical evidence review (Chapter 27, and appendix H).
The aim of the NMA was to calculate treatment specific log odds ratios and relative risks for response to be consistent with the comparative effectiveness results presented elsewhere in the clinical evidence review and for ease of interpretation. Let BO, , and p denote the baseline odds, treatment specific odds, treatment specific log odds ratio and treatment specific absolute probability respectively. Then:
And:
Once the treatment specific probabilities for response are calculated, we divide them by the baseline probability (pb) to get treatment specific relative risks (rrb):
This approach has the advantage that baseline and relative effects are both modelled on the same log odds scale, and also ensures that the uncertainty in the estimation of both baseline and relative effects is accounted for in the model.
We also calculated the overall ranking of interventions according to their relative risk compared to control group. Due to the skewness of the data, the NMA relative risks and rank results are reported as medians rather than means (as in the direct comparisons) to give a more accurate representation of the ‘most likely’ value. The median rank for each intervention was derived from the resulting distribution and these are presented on a rank plot with the associated 95% credible intervals.
A key assumption behind NMA is that the network is consistent. In other words, it is assumed that the direct and indirect treatment effect estimates do not disagree with one another. Discrepancies between direct and indirect estimates of effect may result from several possible causes. First, there is chance and if this is the case then the network meta-analysis results are likely to be more precise as they pool together more data than conventional meta-analysis estimates alone. Second, there could be differences between the trials included in terms of their clinical or methodological characteristics.
This heterogeneity is a problem for network meta-analysis but may be dealt with by subgroup analysis, meta-regression or by carefully defining inclusion criteria. Inconsistency, caused by heterogeneity, was assessed subjectively by comparing the relative risks from the direct evidence (from pair-wise meta-analysis) to the relative risks from the combined direct and indirect evidence (from NMA). We further tested for inconsistency by developing inconsistency models for networks of binary outcomes using the TSD 4 template from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). We compared the posterior mean of the residual deviance between the consistency and inconsistency models to see which was a better fit to the data (closest to the number of trial arms in each network) and checked the difference in deviance information criterion (DIC) values between the two models was small (less than 3–5) or if it was larger, that the smaller DIC and hence better fitting model was the consistency model. No inconsistency was identified.
M.2.3. Results
M.2.3.1. Deep vein thrombosis (symptomatic and asymptomatic)
Included studies
26 studies were identified as reporting on DVT (symptomatic and asymptomatic) outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 23 studies involving 19 treatments were included in the network for DVT. The network can be seen in Figure 833 and the trial data for each of the studies included in the NMA are presented in Table 248.

Figure 833Network diagram for DVT
Table 248Study data for DVT network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Intervention 3 | Comparison | Intervention 1 | Intervention 2 | Intervention 3 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | |||||||
| Chin 2009177 | No prophylaxis | LMWH (standard dose; standard duration) | AES (length unspecified) | IPCD (length unspecified) | 24 | 110 | 6 | 110 | 14 | 110 | 9 | 110 |
| Leclerc 1992543 | No prophylaxis | LMWH (high dose; standard duration) | - | - | 37 | 64 | 11 | 65 | - | - | - | - |
| Wilson 19921014 | No prophylaxis | Foot pump | - | - | 19 | 32 | 5 | 28 | - | - | - | - |
| Fuji 2010320 | No prophylaxis | Dabigatran | - | - | 57 | 101 | 23 | 96 | - | - | - | - |
| Blanchard 1999A106 | LMWH (standard dose; standard duration) | IPCD (length unspecified) | - | - | 16 | 67 | 34 | 63 | - | - | - | - |
| Norgren 1998700 | LMWH (standard dose; standard duration) | Foot pump + AES | - | - | 0 | 14 | 4 | 15 | - | - | - | - |
| Zou 20141052 | LMWH (standard dose; standard duration) | Rivaroxaban | Aspirin | - | 14 | 112 | 3 | 102 | 18 | 110 | - | - |
| Lassen 2008525 | LMWH (standard dose; standard duration) | Rivaroxaban | - | - | 160 | 878 | 79 | 824 | - | - | - | - |
| Eriksson 2007293 | LMWH (standard dose; standard duration) | Dabigatran | - | - | 192 | 685 | 182 | 675 | - | - | - | - |
| Comp 2001208 | LMWH (standard dose; standard duration) | LMWH (standard duration; extended duration) | - | - | 37 | 144 | 33 | 155 | - | - | - | - |
| Lassen 2010535 | LMWH (standard dose; standard duration) | Apixaban | - | - | 243 | 997 | 142 | 971 | - | - | - | - |
| Turpie 2009956 | LMWH (high dose; standard duration) | Rivaroxaban | - | - | 86 | 959 | 61 | 965 | - | - | - | - |
| Ginsberg 2009792 | LMWH (high dose; standard duration) | Dabigatran | - | - | 158 | 643 | 181 | 604 | - | - | - | - |
| Lassen 2007532 | LMWH (high dose; standard duration) | Apixaban | VKA | - | 15 | 109 | 21 | 208 | 29 | 109 | - | - |
| Lassen 2009536 | LMWH (high dose; standard duration) | Apixaban | - | - | 92 | 1122 | 89 | 1142 | - | - | - | - |
| Fitzgerald 2001308 | LMWH (high dose; standard duration) | VKA | - | - | 44 | 173 | 79 | 176 | - | - | - | - |
| Leclerc 1996544 | LMWH (high dose; standard duration) | VKA | - | - | 76 | 206 | 109 | 211 | - | - | - | - |
| Colwell 1995D205 | LMWH (high dose; standard duration) | UFH | - | - | 56 | 145 | 77 | 143 | - | - | - | - |
| Cho 2013178 | AES (length unspecified) | Fondaparinux + AES | - | - | 19 | 74 | 5 | 74 | - | - | - | - |
| Fuji 2008A328 | AES (length unspecified) | LMWH (standard dose; standard duration) + AES | LMWH low dose; standard duration) + AES | - | 48 | 79 | 34 | 78 | 26 | 74 | - | - |
| Warwick 2002995 | Foot pump + AES | LMWH (standard dose; standard duration) + AES | - | - | 57 | 99 | 48 | 89 | - | - | - | - |
| Bauer 200178 | Fondaparinux + AES | LMWH (high dose; standard duration) + AES | - | - | 45 | 361 | 98 | 361 | - | - | - | - |
| Fauno 1994301 | LMWH (standard dose; standard duration) + AES | UFH + AES | - | - | 21 | 91 | 25 | 93 | - | - | - | - |
N; number of events, NA; number analysed
NMA results - DVT
Table 249 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 249Risk ratios for DVT (symptomatic and asymptomatic)
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no prophylaxis | LMWH (standard dose; standard duration) | 0.25 (0.11, 0.59) | 0.26 (0.15, 0.43) |
| LMWH (high dose; standard duration) | 0.29 (0.16, 0.52) | 0.18 (0.10, 0.30) | |
| AES (length unspecified) | 0.58 (0.32, 1.07) | 0.88 (0.55, 1.56) | |
| Dabigatran | 0.42 (0.29, 0.63) | 0.25 (0.14, 0.42) | |
| IPCD (length unspecified) | 0.38 (0.18, 0.77) | 0.61 (0.32, 1.04) | |
| Foot pump | 0.30 (0.13, 0.70) | 0.20 (0.05, 0.63) | |
| Foot pump + AES | - | 0.55 (0.25, 1.48) | |
| Rivaroxaban | - | 0.12 (0.06, 0.22) | |
| Aspirin | - | 0.41 (0.16, 0.94) | |
| LMWH (standard dose; extended duration) | - | 0.21 (0.08, 0.49) | |
| Apixaban | - | 0.15 (0.07, 0.26) | |
| VKA | - | 0.35 (0.17, 0.65) | |
| UFH | - | 0.31 (0.13, 0.69) | |
| Fondaparinux + AES | - | 0.35 (0.16, 0.67) | |
| LMWH (standard dose; standard duration) + AES | - | 0.42 (0.24, 1.00) | |
| LMWH (low dose; standard duration) + AES | - | 0.56 (0.26, 1.32) | |
| LMWH high dose; standard duration) + AES | - | 0.77 (0.31, 1.57) | |
| UFH + AES | - | 0.50 (0.19, 1.50) | |
| Versus LMWH (standard dose; standard duration) | LMWH (high dose; standard duration) | - | 0.69 (0.44, 1.05) |
| AES (length unspecified) | 2.33 (0.93, 5.85)* | 3.45 (1.83, 7.10) | |
| Dabigatran | 1.29 (1.09, 1.53)* | 0.97 (0.64, 1.52) | |
| IPCD (length unspecified) | 2.05 (1.32, 3.17)* | 2.33 (1.31, 4.19) | |
| Foot pump | - | 0.77 (0.18, 2.70) | |
| Foot pump + AES | 8.44 (0.50, 143.77)* | 2.15 (0.81, 6.66) | |
| Rivaroxaban | 0.50 (0.39, 0.64)* | 0.46 (0.28, 0.70) | |
| Aspirin | 1.31 (0.69, 2.50)* | 1.59 (0.71, 3.32) | |
| LMWH (standard dose; extended duration) | 0.83 (0.55, 1.25) | 0.80 (0.38, 1.63) | |
| Apixaban | 0.60 (0.50, 0.72)* | 0.57 (0.35, 0.88) | |
| VKA | - | 1.33 (0.71, 2.43) | |
| UFH | - | 1.21 (0.54, 2.59) | |
| Fondaparinux + AES | - | 1.35 (0.68, 2.59) | |
| LMWH (standard dose; standard duration) + AES | - | 1.67 (0.70, 4.69) | |
| LMWH (low dose; standard duration) + AES | - | 2.17 (0.87, 5.97) | |
| LMWH high dose; standard duration) + AES | - | 2.94 (1.25, 6.49) | |
| UFH + AES | - | 1.97 (0.62, 6.92) | |
| Versus LMWH (high dose; standard duration) | AES (length unspecified) | - | 5.04 (2.52, 10.94) |
| Dabigatran | 1.22 (1.02, 1.46)* | 1.41 (0.93, 2.26) | |
| IPCD (length unspecified) | - | 3.40 (1.74, 6.70) | |
| Foot pump | - | 1.13 (0.26, 3.98) | |
| Foot pump + AES | - | 3.13 (1.10, 10.34) | |
| Rivaroxaban | 0.70 (0.51, 0.97)* | 0.67 (0.39, 1.06) | |
| Aspirin | - | 2.31 (0.96, 5.32) | |
| LMWH (standard dose; extended duration) | - | 1.16 (0.49, 2.69) | |
| Apixaban | 0.99 (0.77, 1.28)* | 0.82 (0.53, 1.25) | |
| VKA | 1.58 (1.33, 1.87)* | 1.94 (1.23, 3.06) | |
| UFH | 1.39 (1.08, 1.80)* | 1.76 (0.89, 3.38) | |
| Fondaparinux + AES | - | 1.97 (1.02, 3.71) | |
| LMWH (standard dose; standard duration) + AES | - | 2.43 (0.96, 7.27) | |
| LMWH (low dose; standard duration) + AES | - | 3.17 (1.21, 9.19) | |
| LMWH high dose; standard duration) + AES | - | 4.27 (1.86, 9.50) | |
| UFH + AES | - | 2.88 (0.86, 10.61) | |
| Versus AES (length unspecified) | Dabigatran | - | 0.28 (0.13, 0.56) |
| IPCD (length unspecified) | 0.64 (0.29, 1.42) | 0.68 (0.32, 1.23) | |
| Foot pump | - | 0.22 (0.05, 0.82) | |
| Foot pump + AES | - | 0.62 (0.29, 1.46) | |
| Rivaroxaban | - | 0.13 (0.05, 0.28) | |
| Aspirin | - | 0.46 (0.16, 1.12) | |
| LMWH (standard dose; extended duration) | - | 0.23 (0.08, 0.59) | |
| Apixaban | - | 0.16 (0.07, 0.34) | |
| VKA | - | 0.39 (0.16, 0.82) | |
| UFH | - | 0.35 (0.12, 0.84) | |
| Fondaparinux + AES | 0.26 (0.11, 0.67) | 0.39 (0.17, 0.76) | |
| LMWH (standard dose; standard duration) + AES | 0.58 (0.40, 0.83) | 0.48 (0.29, 0.93) | |
| LMWH (low dose; standard duration) + AES | 0.72 (0.53, 0.98) | 0.63 (0.32, 1.21) | |
| LMWH high dose; standard duration) + AES | - | 0.87 (0.34, 1.70) | |
| UFH + AES | - | 0.57 (0.23, 1.47) | |
| Versus Dabigatran | IPCD (length unspecified) | - | 2.39 (1.22, 4.66) |
| Foot pump | - | 0.79 (0.18, 2.76) | |
| Foot pump + AES | - | 2.20 (0.79, 7.17) | |
| Rivaroxaban | - | 0.47 (0.25, 0.79) | |
| Aspirin | - | 1.63 (0.66, 3.73) | |
| LMWH (standard dose; extended duration) | - | 0.82 (0.34, 1.86) | |
| Apixaban | - | 0.58 (0.33, 0.97) | |
| VKA | - | 1.37 (0.72, 2.51) | |
| UFH | - | 1.24 (0.54, 2.65) | |
| Fondaparinux + AES | - | 1.39 (0.66, 2.76) | |
| LMWH (standard dose; standard duration) + AES | - | 1.71 (0.68, 5.04) | |
| LMWH (low dose; standard duration) + AES | - | 2.23 (0.85, 6.41) | |
| LMWH high dose; standard duration) + AES | - | 3.01 (1.23, 6.91) | |
| UFH + AES | - | 2.02 (0.61, 7.35) | |
| Versus IPCD (length unspecified) | Foot pump | - | 0.33 (0.07, 1.21) |
| Foot pump + AES | - | 0.91 (0.36, 2.87) | |
| Rivaroxaban | - | 0.20 (0.09, 0.40) | |
| Aspirin | - | 0.68 (0.25, 1.68) | |
| LMWH (standard dose; extended duration) | - | 0.34 (0.13, 0.85) | |
| Apixaban | - | 0.24 (0.12, 0.48) | |
| VKA | - | 0.57 (0.26, 1.24) | |
| UFH | - | 0.52 (0.20, 1.28) | |
| Fondaparinux + AES | - | 0.58 (0.26, 1.26) | |
| LMWH (standard dose; standard duration) + AES | - | 0.70 (0.33, 1.99) | |
| LMWH (low dose; standard duration) + AES | - | 0.93 (0.39, 2.55) | |
| LMWH high dose; standard duration) + AES | - | 1.26 (0.49, 3.00) | |
| UFH + AES | - | 0.84 (0.28, 2.90) | |
| Versus foot pump | Foot pump + AES | - | 2.80 (0.62, 17.30) |
| Rivaroxaban | - | 0.59 (0.16, 2.65) | |
| Aspirin | - | 2.06 (0.46, 10.59) | |
| LMWH (standard dose; extended duration) | - | 1.04 (0.24, 5.28) | |
| Apixaban | - | 0.73 (0.20, 3.27) | |
| VKA | - | 1.73 (0.45, 8.09) | |
| UFH | - | 1.57 (0.37, 7.75) | |
| Fondaparinux + AES | - | 1.75 (0.45, 8.29) | |
| LMWH (standard dose; standard duration) + AES | - | 2.18 (0.52, 12.54) | |
| LMWH (low dose; standard duration) + AES | - | 2.83 (0.66, 16.01) | |
| LMWH high dose; standard duration) + AES | - | 3.81 (0.90, 19.29) | |
| UFH + AES | - | 2.57 (0.51, 17.00) | |
| Versus foot pump + AES | Rivaroxaban | - | 0.21 (0.06, 0.63) |
| Aspirin | - | 0.74 (0.19, 2.29) | |
| LMWH (standard dose; extended duration) | - | 0.37 (0.09, 1.24) | |
| Apixaban | - | 0.26 (0.08, 0.76) | |
| VKA | - | 0.62 (0.18, 1.77) | |
| UFH | - | 0.56 (0.14, 1.76) | |
| Fondaparinux + AES | - | 0.63 (0.19, 1.75) | |
| LMWH (standard dose; standard duration) + AES | 0.94 (0.73, 1.21) | 0.77 (0.42, 1.48) | |
| LMWH (low dose; standard duration) + AES | - | 1.01 (0.39, 2.44) | |
| LMWH high dose; standard duration) + AES | - | 1.39 (0.38, 3.64) | |
| UFH + AES | - | 0.92 (0.34, 2.33) | |
| Versus Rivaroxaban | Aspirin | - | 3.47 (1.53, 7.98) |
| LMWH (standard dose; extended duration) | - | 1.74 (0.74, 4.22) | |
| Apixaban | - | 1.24 (0.71, 2.25) | |
| VKA | - | 2.91 (1.54, 5.91) | |
| UFH | - | 2.64 (1.18, 6.17) | |
| Fondaparinux + AES | - | 2.96 (1.40, 6.43) | |
| LMWH (standard dose; standard duration) + AES | - | 3.67 (1.34, 11.97) | |
| LMWH (low dose; standard duration) + AES | - | 4.78 (1.72, 15.07) | |
| LMWH high dose; standard duration) + AES | - | 6.43 (2.61, 16.07) | |
| UFH + AES | - | 4.35 (1.24, 17.22) | |
| Versus Aspirin | LMWH (standard dose; extended duration) | - | 0.50 (0.17, 1.47) |
| Apixaban | - | 0.36 (0.15, 0.86) | |
| VKA | - | 0.84 (0.33, 2.22) | |
| UFH | - | 0.76 (0.26, 2.25) | |
| Fondaparinux + AES | - | 0.85 (0.32, 2.34) | |
| LMWH (standard dose; standard duration) + AES | - | 1.04 (0.37, 3.85) | |
| LMWH (low dose; standard duration) + AES | - | 1.37 (0.45, 4.90) | |
| LMWH high dose; standard duration) + AES | - | 1.85 (0.62, 5.60) | |
| UFH + AES | - | 1.24 (0.34, 5.42) | |
| Versus LMWH (standard dose; extended duration) | Apixaban | - | 0.71 (0.30, 1.69) |
| VKA | - | 1.67 (0.65, 4.43) | |
| UFH | - | 1.52 (0.52, 4.47) | |
| Fondaparinux + AES | - | 1.70 (0.63, 4.61) | |
| LMWH (standard dose; standard duration) + AES | - | 2.09 (0.68, 7.77) | |
| LMWH (low dose; standard duration) + AES | - | 2.73 (0.86, 9.91) | |
| LMWH high dose; standard duration) + AES | - | 3.69 (1.22, 11.11) | |
| UFH + AES | - | 2.49 (0.64, 10.94) | |
| Versus Apixaban | VKA | - | 2.35 (1.29, 4.42) |
| UFH | - | 2.14 (0.97, 4.67) | |
| Fondaparinux + AES | - | 2.39 (1.25, 4.54) | |
| LMWH (standard dose; standard duration) + AES | - | 2.96 (1.13, 9.12) | |
| LMWH (low dose; standard duration) + AES | - | 3.85 (1.43, 11.47) | |
| LMWH high dose; standard duration) + AES | - | 5.19 (2.26, 11.67) | |
| UFH + AES | - | 3.49 (1.02, 13.17) | |
| Versus VKA | UFH | - | 0.91 (0.40, 1.99) |
| Fondaparinux + AES | - | 1.01 (0.47, 2.18) | |
| LMWH (standard dose; standard duration) + AES | - | 1.24 (0.49, 3.95) | |
| LMWH (low dose; standard duration) + AES | - | 1.62 (0.60, 5.06) | |
| LMWH high dose; standard duration) + AES | - | 2.20 (0.88, 5.40) | |
| UFH + AES | - | 1.47 (0.44, 5.73) | |
| Versus UFH | Fondaparinux + AES | - | 1.12 (0.45, 2.81) |
| LMWH (standard dose; standard duration) + AES | - | 1.37 (0.48, 4.98) | |
| LMWH (low dose; standard duration) + AES | - | 1.80 (0.60, 6.29) | |
| LMWH high dose; standard duration) + AES | - | 2.42 (0.87, 6.89) | |
| UFH + AES | - | 1.62 (0.45, 7.00) | |
| Versus Fondaparinux + AES | LMWH (standard dose; standard duration) + AES | - | 1.23 (0.51, 3.73) |
| LMWH (low dose; standard duration) + AES | - | 1.61 (0.63, 4.71) | |
| LMWH high dose; standard duration) + AES | 2.18 (1.58, 3.00) | 2.17 (1.26, 3.79) | |
| UFH + AES | - | 1.46 (0.45, 5.43) | |
| Versus LMWH (standard dose; standard duration) + AES | LMWH (low dose; standard duration) + AES | 1.24 (0.83, 1.85) | 1.31 (0.61, 2.48) |
| LMWH high dose; standard duration) + AES | - | 1.81 (0.55, 3.92) | |
| UFH + AES | - | 1.19 (0.54, 2.35) | |
| Versus LMWH (low dose; standard duration) + AES | LMWH high dose; standard duration) + AES | - | 1.37 (0.43, 3.45) |
| UFH + AES | - | 0.91 (0.33, 2.51) | |
| Versus LMWH (high dose; standard duration) + AES | UFH + AES | - | 0.66 (0.22, 2.60) |
- *
Intervention and comparison have been switched in Review Manager
Figure 834 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 19 different interventions being evaluated.

Figure 834Rank order for interventions based on the relative risk of experiencing DVT
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 352 compared with 350 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 51 reported. This corresponds well to the total number of trial arms, 51. The DIC statistics were as follows in Table 250. The between trial standard deviation in the random effects analysis was 0.24 (95% CI 0.09 to 0.56). On evaluating inconsistency by comparing risk ratios, three inconsistencies were identified. Firstly, the NMA estimated risk ratio for VKA compared to LMWH at a high dose and standard duration (1.94 [1.23, 3.06]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (1.58 [1.33, 1.87]). Secondly, the NMA estimated risk ratio for dabigatran versus no prophylaxis (0.25 [0.14, 0.42]) lay outside of the confidence interval of the risk ration estimated for the direct comparison (0.42 [0.29, 0.63]). Lastly, the NMA estimated risk ratio for dabigatran compared to LMWH at a standard dose and standard duration (0.97 [0.64, 1.52]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (1.29 [1.09, 1.53]) An inconsistency model was run and the DIC statistics were as follows in Table 250. The difference in the DIC is small (<3–5) with the consistency model having the lower DIC value. This suggests that it fits the data better than the inconsistency model.
Table 250Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – DVT
| DIC | ResDev | |
|---|---|---|
| Consistency model | 352.435 | 51 |
| Inconsistency model | 357.161 | 51 |
M.2.3.2. Pulmonary embolism
Included studies
19 studies were identified as reporting on major bleeding outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 12 studies involving 13 treatments were included in the network for PE. The network can be seen in Figure 835 and the trial data for each of the studies included in the NMA are presented in Table 251.

Figure 835Network diagram for PE
Table 251Study data for PE network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Intervention 3 | Comparison | Intervention 1 | Intervention 2 | Intervention 3 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | N | NA | |||||
| Chin 2009177 | No prophylaxis | LMWH (standard dose; standard duration) | AES (length unspecified) | IPCD (length unspecified) | 1 | 110 | 0 | 110 | 1 | 110 | 0 | 110 |
| Lassen 2008525 | LMWH (standard dose; standard duration) | Rivaroxaban | - | - | 4 | 1217 | 0 | 1201 | - | - | - | - |
| Lassen 2010535 | LMWH (standard dose; standard duration) | Apixaban | - | - | 1 | 1449 | 3 | 1458 | - | - | - | - |
| Comp 2001208 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | - | 2 | 222 | 0 | 218 | - | - | - | - |
| Fuji 2008A328 | AES | LMWH (standard dose; standard duration) + AES | LMWH (low dose; standard duration) + AES | - | 1 | 79 | 1 | 74 | 1 | 78 | - | - |
| Ginsberg 2009792 | Dabigatran | LMWH (high dose; standard duration) | - | - | 6 | 604 | 5 | 643 | - | - | - | - |
| Turpie 2009956 | Rivaroxaban | LMWH (high dose; standard duration) | - | - | 4 | 1526 | 8 | 1508 | - | - | - | - |
| Lassen 2009536 | Apixaban | LMWH (high dose; standard duration) | - | - | 15 | 1599 | 10 | 1596 | - | - | - | - |
| Lassen 2007532 | Apixaban | LMWH (high dose; standard duration) | VKA | - | 0 | 208 | 2 | 109 | 0 | 109 | - | - |
| Fitzgerald 2001308 | LMWH (high dose; standard duration) | VKA | - | - | 0 | 173 | 1 | 176 | - | - | - | - |
| Leclerc 1996543 | LMWH (high dose; standard duration) | VKA | - | - | 1 | 206 | 3 | 211 | - | - | - | - |
| Colwell 1995D205 | LMWH (high dose; standard duration) | UFH | - | - | 0 | 145 | 2 | 143 | - | - | - | - |
N; number of events, NA; number analysed
NMA results - PE
Table 252 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 252Risk ratios for PE
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no prophylaxis | LMWH (standard dose; standard duration) | 0.33 (0.01, 8.09) | 0.20 (0.00, 8.57) |
| AES (length unspecified) | 1.00 (0.06, 15.79) | 0.98 (0.04, 24.95) | |
| IPCD (length unspecified) | 0.33 (0.01, 8.09) | 0.20 (0.00, 8.53) | |
| Dabigatran | - | 0.47 (0.00, 56.97) | |
| Rivaroxaban | - | 0.08 (0.00, 6.65) | |
| Apixaban | - | 0.52 (0.00, 36.43) | |
| LMWH (standard duration; extended duration) | - | 0.02 (0.00, 3.86) | |
| LMWH (standard dose; standard duration) + AES | - | 1.00 (0.01, 199.30) | |
| LMWH (low dose; standard duration) + AES | - | 0.97 (0.01, 167.70) | |
| LMWH (high dose; standard duration) | - | 0.37 (0.00, 30.66) | |
| VKA | - | 0.63 (0.00, 64.93) | |
| UFH | - | 1.79 (0.00, 625.00) | |
| Versus LMWH (standard dose; standard duration) | AES (length unspecified) | 3.00 (0.12, 72.85)* | 5.00 (0.12, 3120.00) |
| IPCD (length unspecified) | - | 0.98 (0.00, 791.60) | |
| Dabigatran | - | 2.45 (0.11, 52.27) | |
| Rivaroxaban | 0.11 (0.01, 2.03)* | 0.45 (0.04, 3.62) | |
| Apixaban | 6.00 (0.72, 49.81)* | 2.59 (0.32, 21.68) | |
| LMWH (standard duration; extended duration) | 0.20 (0.01, 4.22) | 0.11 (0.00, 3.33) | |
| LMWH (standard dose; standard duration) + AES | - | 6.04 (0.02, 9283.00) | |
| LMWH (low dose; standard duration) + AES | - | 5.68 (0.02, 8979.00) | |
| LMWH (high dose; standard duration) | - | 1.90 (0.20, 18.92) | |
| VKA | - | 3.23 (0.20, 52, 24) | |
| UFH | - | 9.06 (0.12, 1640.00) | |
| Versus AES (length unspecified) | IPCD (length unspecified) | 0.33 (0.01, 8.09) | 0.20 (0.00, 8.36) |
| Dabigatran | - | 0.48 (0.00, 48.08) | |
| Rivaroxaban | - | 0.08 (0.00, 6.65) | |
| Apixaban | - | 0.52 (0.00, 32.84) | |
| LMWH (standard duration; extended duration) | - | 0.01 (0.00, 3.86) | |
| LMWH (standard dose; standard duration) + AES | 1.07 (0.07, 16.76) | 1.04 (0.02, 61.02) | |
| LMWH (low dose; standard duration) + AES | 1.01 (0.06, 15.91) | 1.00 (0.02, 54.60) | |
| LMWH (high dose; standard duration) | - | 0.37 (0.00, 27.68) | |
| VKA | - | 0.64 (0.00, 52.48) | |
| UFH | - | 1.95 (0.00, 372.20) | |
| Versus IPCD (length unspecified) | Dabigatran | - | 2.51 (0.00, 3274.00) |
| Rivaroxaban | - | 0.45 (0.00, 447.00) | |
| Apixaban | - | 2.68 (0.00, 2584.00) | |
| LMWH (standard duration; extended duration) | - | 0.08 (0.00, 189.20) | |
| LMWH (standard dose; standard duration) + AES | - | 5.96 (0.02, 9804.00) | |
| LMWH (low dose; standard duration) + AES | - | 5.55 (0.02, 8305.00) | |
| LMWH (high dose; standard duration) | - | 1.96 (0.00, 2030.00) | |
| VKA | - | 3.31 (0.00, 3828.00) | |
| UFH | - | 10.55 (0.00, 26060.00) | |
| Versus Dabigatran | Rivaroxaban | - | 0.18 (0.01, 2.80) |
| Apixaban | - | 1.07 (0.08, 14.05) | |
| LMWH (standard duration; extended duration) | - | 0.04 (0.00, 4.37) | |
| LMWH (standard dose; standard duration) + AES | - | 2.40 (0.01, 7128.00) | |
| LMWH (low dose; standard duration) + AES | - | 2.28 (0.00, 6754.00) | |
| LMWH (high dose; standard duration) | 0.78 (0.24, 2.55) | 0.79 (0.10, 6.71) | |
| VKA | - | 1.31 (0.09, 21.28) | |
| UFH | - | 3.52 (0.05, 769.80) | |
| Versus Rivaroxaban | Apixaban | - | 5.92 (0.73, 64.04) |
| LMWH (standard duration; extended duration) | - | 0.23 (0.00, 16.74) | |
| LMWH (standard dose; standard duration) + AES | - | 14.28 (0.03, 35160.00) | |
| LMWH (low dose; standard duration) + AES | - | 13.27 (0.03, 32390.00) | |
| LMWH (high dose; standard duration) | 2.02 (0.61, 6.71) | 4.23 (0.73, 37.87) | |
| VKA | - | 7.32 (0.65, 116.30) | |
| UFH | - | 20.27 (0.35, 4323.00) | |
| Versus Apixaban | LMWH (standard duration; extended duration) | - | 0.04 (0.00, 2.29) |
| LMWH (standard dose; standard duration) + AES | - | 2.21 (0.01, 4884.00) | |
| LMWH (low dose; standard duration) + AES | - | 2.11 (0.01, 4578.00) | |
| LMWH (high dose; standard duration) | 0.44 (0.18, 1.06) | 0.72 (0.17, 3.46) | |
| VKA | - | 1.22 (0.15, 10.54) | |
| UFH | - | 3.25 (0.06, 574.10) | |
| Versus LMWH (standard dose; extended duration) | LMWH (standard dose; standard duration) + AES | - | 79.99 (0.07, 785700.00) |
| LMWH (low dose; standard duration) + AES | - | 74.78 (0.06, 724000.00) | |
| LMWH (high dose; standard duration) | - | 19.13 (0.30, 21100.00) | |
| VKA | - | 33.28 (0.38, 43380.00) | |
| UFH | - | 111.30 (0.35, 330100.00) | |
| Versus LMWH (standard dose; standard duration) + AES | LMWH (low dose; standard duration) + AES | 0.95 (0.06, 14.89) | 0.95 (0.01, 47.24) |
| LMWH (high dose; standard duration) | - | 0.32 (0.00, 99.27) | |
| VKA | - | 0.56 (0.00, 140.60) | |
| UFH | - | 1.97 (0.00, 218.00) | |
| Versus LMWH (low dose; standard duration) + AES | LMWH (high dose; standard duration) | - | 0.34 (0.00, 135.20) |
| VKA | - | 0.59 (0.00, 249.50) | |
| UFH | - | 1.94 (0.00, 1050.00) | |
| Versus LMWH (high dose; standard duration) | VKA | 1.31 (0.30, 5.79)* | 1.68 (0.29, 10.18) |
| UFH | 3.04 (0.12, 74.05)* | 4.38 (0.12, 663.70) | |
| Versus VKA | UFH | - | 2.61 (0.04, 533. 70) |
- *
Intervention and comparison have been switched in Review Manager
Figure 836 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 13 different interventions being evaluated.

Figure 836Rank order for interventions based the relative risk of experiencing PE
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 125 compared with 127 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 32 reported. This corresponds well to the total number of trial arms, 28. The between trial standard deviation in the random effects analysis was 0.67 (95% CI 0.18 to 1.98). No inconsistency was identified between the direct RR and NMA results. The DIC statistics were as follows in Table 253.
Table 253Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – PE
| DIC | ResDev | |
|---|---|---|
| Consistency model | 124.870 | 32 |
| Inconsistency model | 125.068 | 32 |
M.2.3.3. Major bleeding
Included studies
19 studies were identified as reporting on major bleeding outcomes. All of the studies identified, involving 11 treatments were included in the network for major bleeding. The network can be seen in Figure 837 and the trial data for each of the studies included in the NMA are presented in Table 254.

Figure 837Network diagram for major bleeding
Table 254Study data for major bleeding network meta-analysis
| Study | Comparison | Intervention 1 | Intervention 2 | Comparison | Intervention 1 | Intervention 2 | |||
|---|---|---|---|---|---|---|---|---|---|
| N | NA | N | NA | N | NA | ||||
| Fuji 2008A328 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | LMWH (low dose; standard duration) | 4 | 89 | 1 | 91 | 0 | 89 |
| Chin 2009177 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | - | 0 | 110 | 2 | 110 | - | - |
| Blanchard 1999A106 | No prophylaxis/mechanical | LMWH (standard dose; standard duration) | - | 0 | 63 | 1 | 67 | - | - |
| Leclerc 1992543 | No prophylaxis/mechanical | LMWH (high dose; standard duration) | - | 1 | 65 | 0 | 66 | - | - |
| Fuji 2008325 | No prophylaxis/mechanical | Fondaparinux | - | 1 | 87 | 1 | 84 | - | - |
| Fuji 2010320 | No prophylaxis/mechanical | Dabigatran | - | 1 | 124 | 4 | 129 | - | - |
| Lassen 2010535 | LMWH (standard dose; standard duration) | Apixaban | - | 14 | 1508 | 9 | 1501 | - | - |
| Eriksson 2007293 | LMWH (standard dose; standard duration) | Dabigatran | - | 9 | 694 | 10 | 679 | - | - |
| Mirdami di 2014641 | LMWH (standard dose; standard duration) | Dabigatran | - | 2 | 45 | 3 | 45 | - | - |
| Lassen 2008525 | LMWH (standard dose; standard duration) | Rivaroxaban | - | 17 | 1277 | 21 | 1254 | - | - |
| Comp 2001208 | LMWH (standard dose; standard duration) | LMWH (standard dose; extended duration) | - | 1 | 221 | 0 | 217 | - | - |
| Bauer 200178 | LMWH (high dose; standard duration) | Fondaparinux | - | 1 | 517 | 11 | 517 | - | - |
| Lassen 2009536 | LMWH (high dose; standard duration) | Apixaban | - | 22 | 1588 | 11 | 1596 | - | - |
| Lassen 2007532 | LMWH (high dose; standard duration) | Apixaban | VKA | 0 | 149 | 4 | 305 | 0 | 151 |
| Ginsberg 2009792 | LMWH (high dose; standard duration) | Dabigatran | - | 12 | 868 | 5 | 857 | - | - |
| Turpie 2009956 | LMWH (high dose; standard duration) | Rivaroxaban | - | 16 | 1564 | 27 | 1584 | - | - |
| Colwell 1995D205 | LMWH (high dose; standard duration) | UFH | - | 3 | 228 | 3 | 225 | - | - |
| Fitzgerald 2001308 | LMWH (high dose; standard duration) | VKA | - | 9 | 173 | 4 | 176 | - | - |
| Leclerc 1996544 | LMWH (high dose; standard duration) | VKA | - | 6 | 336 | 5 | 334 | - | - |
N; number of events, NA; number analysed
NMA results- major bleeding
Table 255 summarises the results of the conventional meta-analyses in terms of odd ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of odd ratios for every possible treatment comparison. Relative risks were not calculated for this outcome as data was only available for non-surgical site bleeding (intracranial haemorrhage + gastrointestinal bleeding) from the observational study used as the source of baseline risk.450
Table 255Odd ratios for major bleeding
| Intervention | Direct (mean with 95% confidence interval) | NMA (median with 95% credible interval) | |
|---|---|---|---|
| Versus no mechanical prophylaxis | LMWH (standard dose; standard duration) | 0.98 (0.28, 3.40) | 1.09 (0.34, 3.75) |
| LMWH (high dose; standard duration) | 0.32 (0.01, 8.08) | 1.02 (0.24, 3.97) | |
| Fondaparinux | 1.04 (0.06, 16.84) | 6.74 (0.79, 76.28) | |
| LMWH (low dose; standard duration) | 0.11 (0.01, 2.00) | 0.08 (0.00, 1.76) | |
| Apixaban | - | 0.79 (0.18, 3.99) | |
| Dabigatran | - | 1.08 (0.29, 4.36) | |
| Rivaroxaban | - | 1.55 (0.32, 7.35) | |
| LMWH (standard dose; extended duration) | - | 0.21 (0.00, 10.41) | |
| UFH | - | 1.03 (0.07, 13.19) | |
| VKA | 0.52 (0.08, 2.89) | ||
| Versus LMWH (standard dose; standard duration) | LMWH (high dose; standard duration) | - | 0.95 (0.27, 2.63) |
| Fondaparinux | - | 6.18 (0.73, 66.87) | |
| LMWH (low dose; standard duration) | 0.34 (0.01, 8.38)* | 0.08 (0.00, 1.62) | |
| Apixaban | 0.64 (0.28, 1.49)* | 0.72 (0.23, 2.50) | |
| Dabigatran | 1.21 (0.54, 2.72)* | 0.99 (0.35, 2.86) | |
| Rivaroxaban | 1.26 (0.66, 2.40)* | 1.43 (0.41, 4.45) | |
| LMWH (standard dose; extended duration) | 0.34 (0.01, 8.34) | 0.19 (0.00, 7.62) | |
| UFH | - | 0.95 (0.07, 10.30) | |
| VKA | - | 0.48 (0.09, 2.05) | |
| Versus LMWH (high dose; standard duration) | Fondaparinux | 11.22 (1.44, 87.20)* | 6.57 (1.07, 62.67) |
| LMWH (low dose; standard duration) | - | 0.08 (0.00, 2.09) | |
| Apixaban | 0.61 (0.31, 1.19)* | 0.77 (0.30, 2.70) | |
| Dabigatran | 0.42 (0.15, 1.19)* | 1.05 (0.35, 3.99) | |
| Rivaroxaban | 1.68 (0.90, 3.13)* | 1.50 (0.49, 5.32) | |
| LMWH (standard dose; extended duration) | - | 0.20 (0.00, 10.27) | |
| UFH | 1.01 (0.20, 5.08)* | 1.01 (0.11, 8.95) | |
| VKA | 0.61 (0.28, 1.37)* | 0.51 (0.15, 1.57) | |
| Versus Fondaparinux | LMWH (low dose; standard duration) | - | 0.01 (0.00, 0.48) |
| Apixaban | - | 0.12 (0.01, 1.08) | |
| Dabigatran | - | 0.16 (0.01, 1.44) | |
| Rivaroxaban | - | 0.23 (0.02, 2.05) | |
| LMWH (standard dose; extended duration) | - | 0.03 (0.00, 2.25) | |
| UFH | - | 0.15 (0.01, 2.68) | |
| VKA | - | 0.08 (0.01, 0.65) | |
| Versus LMWH (low dose; standard duration) | Apixaban | - | 9.71 (0.37, 5795.00) |
| Dabigatran | - | 13.03 (0.54, 7827.00) | |
| Rivaroxaban | - | 18.67 (0.71, 11130.00) | |
| LMWH (standard dose; extended duration) | - | 2.64 (0.00, 3297.00) | |
| UFH | - | 13.32 (0.24, 9936.00) | |
| VKA | 6.30 (0.20, 3743.00) | ||
| Versus Apixaban | Dabigatran | - | 1.36 (0.33, 5.46) |
| Rivaroxaban | - | 1.98 (0.41, 7.59) | |
| LMWH (standard dose; extended duration) | - | 0.26 (0.00, 12.79) | |
| UFH | - | 1.31 (0.10, 13.72) | |
| VKA | 0.22 (0.01, 4.13)* | 0.66 (0.12, 2.53) | |
| Versus Dabigatran | Rivaroxaban | - | 1.45 (0.32, 5.66) |
| LMWH (standard dose; extended duration) | - | 0.19 (0.00, 9.01) | |
| UFH | - | 0.96 (0.07, 10.66) | |
| VKA | 0.48 (0.08, 2.24) | ||
| Versus Rivaroxaban | LMWH (standard dose; extended duration) | - | 0.13 (0.00, 6.77) |
| UFH | - | 0.67 (0.05, 7.67) | |
| VKA | 0.33 (0.06, 1.59) | ||
| Versus LMWH (standard dose; extended duration) | UFH | - | 5.25 (0.05, 3299.00) |
| VKA | 2.51 (0.04, 1310.00) | ||
| Versus UFH | VKA | 0.50 (0.04, 5.92) |
- *
Intervention and comparison have been switched in Review Manager
Figure 838 shows the rank of each intervention compared to the others. The rank indicates the probability of being the best treatment, second best, third best and so on among the 11 different interventions being evaluated.

Figure 838Rank order for interventions based on the relative risk of experiencing major bleeding
SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
Both fixed effects and random effects models were fitted to the data. The random effects model had a DIC of 196 compared with 197 for the fixed effects model. The random effects model used for the NMA is a good fit, with a residual deviance of 41 reported. This corresponds well to the total number of trial arms, 40. The between trial standard deviation in the random effects analysis was 0.54 (95% CI 0.19 to 1.28). No inconsistency was identified between the direct RR and NMA results. The DIC statistics were as follows in Table 256.
Table 256Posterior mean of the residual deviance (resdev) and DIC for the RE network meta-analysis and inconsistency models – Major bleeding
| DIC | TotResDev | |
|---|---|---|
| Consistency model | 196.222 | 42 |
| Inconsistency model | 199.124 | 42 |
M.2.4. Discussion
Based on the results of conventional meta-analyses of direct evidence, as has been previously presented in Chapter 26 and appendix H, deciding upon the most clinical and cost effective prophylaxis intervention in patients undergoing elective knee replacement surgery is challenging. In order to overcome the difficulty of interpreting the conclusions from numerous separate comparisons, network meta-analysis of the direct evidence was performed. The findings of the NMA were used to facilitate the committee in decision-making when developing recommendations.
Our analyses were divided into three critical outcomes. 23 studies informed the DVT network where 19 different individual or combination treatments were evaluated including three mechanical interventions, nine pharmacological interventions, and six interventions that combined both mechanical and pharmacological prophylaxis. 12 studies informed the PE network of 13 different treatments, including two mechanical interventions, seven pharmacological interventions, and two interventions that combined both mechanical and pharmacological prophylaxis. The major bleeding network included 19 studies evaluating 11 treatments, nine of which were pharmacological as for this outcome any mechanical prophylaxis measures were combined with the no prophylaxis intervention as it is believed that mechanical prophylaxis has no associated bleeding risk.
In the DVT network, the top three interventions were rivaroxaban, apixaban and LMWH at a high dose for a standard duration. The bottom three interventions were no prophylaxis, AES (length unspecified) and LMWH at a high dose for a standard duration plus AES. The highest ranked combination of mechanical and pharmacological prophylaxis was fondaparinux plus AES in tenth place. The four other combination interventions of mechanical plus pharmacological interventions ranked from 15 to 17. There was considerable uncertainty about the estimates with the credible intervals for some of the interventions being quite wide. The top three interventions spanned up to 7 rankings.
In the PE network, the top three interventions were LMWH at a standard dose for an extended duration, rivaroxaban, and IPCD (length unspecified). The bottom three interventions were UFH, LMWH at a standard dose for a standard duration plus AES andno prophylaxis. There was also considerable uncertainty in the PE network with wide credible intervals for a majority of the interventions, for example for LMWH at a low dose for a standard duration plus AES and LMWH at a standard dose for a standard duration plus AES spanning all 13 ranking positions.
In the major bleeding network the highest ranked intervention was LMWH at a low dose for a standard duration, followed LMWH at a standard dose for an extended duration then VKA. The bottom three interventions were fondaparinux, rivaroxaban and LMWH at a standard dose for a standard duration. There was a lot of uncertainty within the major bleeding network with very wide credible intervals for all of the interventions spanning almost all ranking positions.
In summary, the three outcomes chosen for analyses were considered to be among the most critical for assessing clinical effectiveness of different VTE prophylaxis strategies. All three networks seemed to fit well, as demonstrated by residual deviance and no obvious inconsistency found in the networks. However the credible intervals around the ranking of treatments in all three networks were wide suggesting considerable uncertainty about these results.
M.2.5. Conclusion
This analysis allowed us to combine findings from many different comparisons presented in the review even when direct comparative data was lacking.
The committee and orthopaedic subgroup noted the wide credible intervals particularly for the PE and major bleeding network meta-analyses. They both also noted that even with the high levels of uncertainty, interventions such as rivaroxaban and LMWH present possible clinical effectiveness in terms of the outcomes of DVT (symptomatic and asymptomatic) and PE.
For details of the rationale and discussion leading to recommendations, please refer to the section linking the evidence to the recommendations (section 27.6, chapter 27).
M.2.6. WinBUGS codes
M.2.6.1. WinBUGS code for number of patients with DVT (symptomatic and asymptomatic)
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[16] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 120639
a <- 16891
for (k in 1:15){ # treatments below 16
logit(v[k]) <- logit(v[16]) - lor[k,16] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 17:NT){ # treatments above 16
logit(v[k]) <- logit(v[16]) + lor[16,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[16] <- v[16]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NT=19, NS=23,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: general physical health indicators
m.tau= -1.26, sd.tau=1.25 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
24 110 6 110 14 110 9 110 NA NA 1 2 4 6 NA 4
37 64 11 65 NA NA NA NA NA NA 1 3 NA NA NA 2
57 101 23 96 NA NA NA NA NA NA 1 5 NA NA NA 2
19 32 5 28 NA NA NA NA NA NA 1 7 NA NA NA 2
192 685 182 675 NA NA NA NA NA NA 2 5 NA NA NA 2
16 67 34 63 NA NA NA NA NA NA 2 6 NA NA NA 2
0.5 15 4.5 16 NA NA NA NA NA NA 2 8 NA NA NA 2
14 112 3 102 18 110 NA NA NA NA 2 9 10 NA NA 3
160 878 79 824 NA NA NA NA NA NA 2 9 NA NA NA 2
37 144 33 155 NA NA NA NA NA NA 2 11 NA NA NA 2
243 997 142 971 NA NA NA NA NA NA 2 12 NA NA NA 2
158 643 181 604 NA NA NA NA NA NA 3 5 NA NA NA 2
86 959 61 965 NA NA NA NA NA NA 3 9 NA NA NA 2
15 109 21 208 29 109 NA NA NA NA 3 12 15 NA NA 3
92 1122 89 1142 NA NA NA NA NA NA 3 12 NA NA NA 2
44 173 79 176 NA NA NA NA NA NA 3 13 NA NA NA 2
76 206 109 211 NA NA NA NA NA NA 3 13 NA NA NA 2
56 145 77 143 NA NA NA NA NA NA 3 14 NA NA NA 2
19 74 5 74 NA NA NA NA NA NA 4 15 NA NA NA 2
48 79 25 74 34 78 NA NA NA NA 4 16 17 NA NA 3
57 99 48 89 NA NA NA NA NA NA 8 16 NA NA NA 2
45 361 98 361 NA NA NA NA NA NA 15 18 NA NA NA 2
21 91 25 93 NA NA NA NA NA NA 16 19 NA NA NA 2
END
list(
d=c(NA,0,0,0,0,0,0,0,1,2,3,4,2,3,1,0,2,1,-2), # one for each treatment
sd.sq=1,
mu=c(0,0,3,0,0, 0,2,0,-1,0, 4,0,3,1,0, 0, 2,1,3, 2,0, 1, 2) )
list(
d=c(NA,1,0,2,0,3,0,0,1,2,3,4,2,3,1,0,1,3,-3), # one for each treatment
sd.sq=0.1,
mu=c(0,2,1,0,-2, 0,3,0,4,0, 2,0,1,3,0, 0, 2,1,3,1,0, 0, -1) )
list(
d=c(NA,0,0,0,0,0,0,0,1,2,3,4,2,3,1,0,0,1,2), # one for each treatment
sd.sq=2,
mu=c(0,3,3,0,4, 0,1,0,-2,0, 1,2,0,2,0, 0, 2,1,3,-3,4, 2, 1) )
M.2.6.2. WinBUGS code for inconsistency model for number of patients with DVT
VTE - inconsistency model - Elective knee DVT ============================== 23 trials 19 treaments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=19,ns=23, m.tau= -1.26, sd.tau=1.25) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 24 110 6 110 14 110 9 110 NA NA 1 2 4 6 NA 4 37 64 11 65 NA NA NA NA NA NA 1 3 NA NA NA 2 57 101 23 96 NA NA NA NA NA NA 1 5 NA NA NA 2 19 32 5 28 NA NA NA NA NA NA 1 7 NA NA NA 2 192 685 182 675 NA NA NA NA NA NA 2 5 NA NA NA 2 16 67 34 63 NA NA NA NA NA NA 2 6 NA NA NA 2 0.5 15 4.5 16 NA NA NA NA NA NA 2 8 NA NA NA 2 14 112 3 102 18 110 NA NA NA NA 2 9 10 NA NA 3 160 878 79 824 NA NA NA NA NA NA 2 9 NA NA NA 2 37 144 33 155 NA NA NA NA NA NA 2 11 NA NA NA 2 243 997 142 971 NA NA NA NA NA NA 2 12 NA NA NA 2 158 643 181 604 NA NA NA NA NA NA 3 5 NA NA NA 2 86 959 61 965 NA NA NA NA NA NA 3 9 NA NA NA 2 15 109 21 208 29 109 NA NA NA NA 3 12 15 NA NA 3 92 1122 89 1142 NA NA NA NA NA NA 3 12 NA NA NA 2 44 173 79 176 NA NA NA NA NA NA 3 13 NA NA NA 2 76 206 109 211 NA NA NA NA NA NA 3 13 NA NA NA 2 56 145 77 143 NA NA NA NA NA NA 3 14 NA NA NA 2 19 74 5 74 NA NA NA NA NA NA 4 15 NA NA NA 2 48 79 25 74 34 78 NA NA NA NA 4 16 17 NA NA 3 57 99 48 89 NA NA NA NA NA NA 8 16 NA NA NA 2 45 361 98 361 NA NA NA NA NA NA 15 18 NA NA NA 2 21 91 25 93 NA NA NA NA NA NA 16 19 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2,1,3,1, 1,2,-3,2,-2, -2,1,1), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0 ), .Dim = c(18,19)) ) # chain 2 list(sd.sq=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0,1,3,1, 1,2,-3,2,0, 0,0,-1), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5 ), .Dim = c(18,19)) ) # chain 3 list(sd.sq=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1,1,3,1, 1,2,-3,2,1, 1,2,2), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3 ), .Dim = c(18,19)) )
M.2.6.3. WinBUGS code for number of patients with pulmonary embolism (PE)
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[9] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 120639
a <- 539
for (k in 1:8){ # treatments below 8
logit(v[k]) <- logit(v[9]) - lor[k,9] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 10:NT){ # treatments above 9
logit(v[k]) <- logit(v[9]) + lor[9,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[9] <- v[9]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 4.
list(NT=13, NS=12,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: general physical health indicators
m.tau= -1.26, sd.tau=1.25 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
1.5 111 0.5 111 1.5 111 0.5 111 NA NA 1 2 3 4 NA 4
4.5 1218 0.5 1202 NA NA NA NA NA NA 2 6 NA NA NA 2
1 1529 7 1528 NA NA NA NA NA NA 2 7 NA NA NA 2
2.5 222 0.5 218 NA NA NA NA NA NA 2 8 NA NA NA 2
1 79 1 74 1 78 NA NA NA NA 3 9 10 NA NA 3
6 604 5 643 NA NA NA NA NA NA 5 11 NA NA NA 2
4 1526 8 1508 NA NA NA NA NA NA 6 11 NA NA NA 2
15 1599 10 1596 NA NA NA NA NA NA 7 11 NA NA NA 2
0.5 209 2.5 110 0.5 110 NA NA NA NA 7 11 12 NA NA 3
0.5 174 1.5 177 NA NA NA NA NA NA 11 12 NA NA NA 2
1 206 3 211 NA NA NA NA NA NA 11 12 NA NA NA 2
0.5 146 1.5 144 NA NA NA NA NA NA 11 13 NA NA NA 2
END
list(
d=c(NA,0,0,0,0,0,0,0,1,2,3,4,2), # one for each treatment
sd.sq=1,
mu=c(0,0,3,0,0, 0,2,0,-1,0, 4,1) )
list(
d=c(NA,1,0,2,0,3,0,0,1,2,3,4,2), # one for each treatment
sd.sq=0.1,
mu=c(0,2,1,0,-2, 0,3,0,4,0, 2,-1) )
list(
d=c(NA,0,0,0,0,0,0,0,1,2,3,4,2), # one for each treatment
sd.sq=2,
mu=c(0,3,3,0,4, 0,1,0,-2,0, 1,0) )
M.2.6.4. WinBUGS code for inconsistency model for number of patients with PE
VTE - inconsistency model - Elective knee PE ============================== 12 studies 13 treaments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=13,ns=12, m.tau= -1.26, sd.tau=1.25) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 1.5 111 0.5 111 1.5 111 0.5 111 NA NA 1 2 3 4 NA 4 4.5 1218 0.5 1202 NA NA NA NA NA NA 2 6 NA NA NA 2 1 1529 7 1528 NA NA NA NA NA NA 2 7 NA NA NA 2 2.5 222 0.5 218 NA NA NA NA NA NA 2 8 NA NA NA 2 1 79 1 74 1 78 NA NA NA NA 3 9 10 NA NA 3 6 604 5 643 NA NA NA NA NA NA 5 11 NA NA NA 2 4 1526 8 1508 NA NA NA NA NA NA 6 11 NA NA NA 2 15 1599 10 1596 NA NA NA NA NA NA 7 11 NA NA NA 2 0.5 209 2.5 110 0.5 110 NA NA NA NA 7 11 12 NA NA 3 0.5 174 1.5 177 NA NA NA NA NA NA 11 12 NA NA NA 2 1 206 3 211 NA NA NA NA NA NA 11 12 NA NA NA 2 0.5 146 1.5 144 NA NA NA NA NA NA 11 13 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0 ), .Dim = c(12,13)) ) # chain 2 list(sd.sq=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5), .Dim = c(12,13)) ) # chain 3 list(sd.sq=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3 ), .Dim = c(12,13)) )
M.2.6.5. WinBUGS code for number of patients with major bleeding
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
#sd ~ dunif(0,5) # vague prior for random effects standard deviation
#tau <- 1/pow(sd,2)
sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var
prec.tau <- pow(sd.tau,-2)
tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance)
sd <- sqrt(sd.sq)
#A ~ dnorm(meanA, precA) # A is on log-odds scale
#precA <- pow(sdA,-2) # turn st dev into precision
v[2] ~ dbeta(a, b) # distribution for prob event on LMWH (std/std)+AES
b <- N-a
N <- 120639
a <- 465
for (k in 1:1){ # treatments below 2
logit(v[k]) <- logit(v[2]) - lor[k,2] # note change in sign
rr[k] <- v[k]/v[1] # calculate relative risk
}
for (k in 3:NT){ # treatments above 2
logit(v[k]) <- logit(v[2]) + lor[2,k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
rr[2] <- v[2]/v[1]
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NT=11, NS=19,
# meanA and sdA are the posterior mean and sd of log-odds of event
#meanA=-1.673, sdA=0.2529,
#Empirical prior Table IV (Turner et al) intervention: Non-Pharma v Pharma;
# outcome type: adverse events
m.tau= -0.84, sd.tau=1.24 )
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[]
4.5 90 1.5 92 0.5 90 NA NA NA NA 1 2 5 NA NA 3
0.5 111 2.5 111 NA NA NA NA NA NA 1 2 NA NA NA 2
0.5 64 1.5 68 NA NA NA NA NA NA 1 2 NA NA NA 2
1.5 66 0.5 67 NA NA NA NA NA NA 1 3 NA NA NA 2
1 87 1 84 NA NA NA NA NA NA 1 4 NA NA NA 2
1 124 4 129 NA NA NA NA NA NA 1 7 NA NA NA 2
14 1508 9 1501 NA NA NA NA NA NA 2 6 NA NA NA 2
9 694 10 679 NA NA NA NA NA NA 2 7 NA NA NA 2
2 45 3 45 NA NA NA NA NA NA 2 7 NA NA NA 2
17 1277 21 1254 NA NA NA NA NA NA 2 8 NA NA NA 2
1.5 222 0.5 218 NA NA NA NA NA NA 2 9 NA NA NA 2
1 517 11 517 NA NA NA NA NA NA 3 4 NA NA NA 2
22 1588 11 1596 NA NA NA NA NA NA 3 6 NA NA NA 2
0.5 150 4.5 306 0.5 152 NA NA NA NA 3 6 11 NA NA 3
12 868 5 857 NA NA NA NA NA NA 3 7 NA NA NA 2
16 1564 27 1584 NA NA NA NA NA NA 3 8 NA NA NA 2
3 228 3 225 NA NA NA NA NA NA 3 10 NA NA NA 2
9 173 4 176 NA NA NA NA NA NA 3 11 NA NA NA 2
6 336 5 334 NA NA NA NA NA NA 3 11 NA NA NA 2
END
list(
d=c(NA,0,0,0,0,0,0,0,1,2,0), # one for each treatment
sd.sq=1,
mu=c(0,0,3,0,0, 0,2,0,-1,0, 4,0,3,1,0,1,3, 2, 1) )
list(
d=c(NA,1,0,2,0,3,0,0,1,2,-2), # one for each treatment
sd.sq=0.1,
mu=c(0,2,1,0,-2, 0,3,0,4,0, 2,0,1,3,0,0,1,0,0) )
list(
d=c(NA,0,0,0,0,0,0,0,1,2,2), # one for each treatment
sd.sq=2,
mu=c(0,3,3,0,4, 0,1,0,-2,0, 1,2,0,2,0,-3,1,2, -1) )
M.2.6.6. WinBUGS code for inconsistency model for number of patients with major bleeding
VTE - inconsistency model - Elective knee MB ============================== 19 trials 11 treaments =============================== # Binomial likelihood, logit link, inconsistency model # Random effects model model{ # *** PROGRAM STARTS for(i in 1:ns){ # LOOP THROUGH STUDIES delta[i,1]<-0 # treatment effect is zero in control arm mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines for (k in 1:na[i]) { # LOOP THROUGH ARMS r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor #Deviance contribution rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k]))) } # summed residual deviance contribution for this trial resdev[i] <- sum(dev[i,1:na[i]]) for (k in 2:na[i]) { # LOOP THROUGH ARMS # trial-specific LOR distributions delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau) } } totresdev <- sum(resdev[]) # Total Residual Deviance for (c in 1:(nt-1)) { # priors for all mean treatment effects for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) } } #sd ~ dunif(0,5) # vague prior for between-trial standard deviation #var <- pow(sd,2) # between-trial variance #tau <- 1/var # between-trial precision sd.sq ~ dlnorm(m.tau,prec.tau) # empirical prior for between-trial Var prec.tau <- pow(sd.tau,-2) tau <- pow(sd.sq,-1) # between-trial precision = (1/between-trial variance) sd <- sqrt(sd.sq) } # *** PROGRAM ENDS Data # DVT # nt=no. treatments, ns=no. studies list(nt=11,ns=19, m.tau= -0.84, sd.tau=1.24) r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] r[,4] n[,4] r[,5] n[,5] t[,1] t[,2] t[,3] t[,4] t[,5] na[] 4.5 90 1.5 92 0.5 90 NA NA NA NA 1 2 5 NA NA 3 0.5 111 2.5 111 NA NA NA NA NA NA 1 2 NA NA NA 2 0.5 64 1.5 68 NA NA NA NA NA NA 1 2 NA NA NA 2 1.5 66 0.5 67 NA NA NA NA NA NA 1 3 NA NA NA 2 1 87 1 84 NA NA NA NA NA NA 1 4 NA NA NA 2 1 124 4 129 NA NA NA NA NA NA 1 7 NA NA NA 2 14 1508 9 1501 NA NA NA NA NA NA 2 6 NA NA NA 2 9 694 10 679 NA NA NA NA NA NA 2 7 NA NA NA 2 2 45 3 45 NA NA NA NA NA NA 2 7 NA NA NA 2 17 1277 21 1254 NA NA NA NA NA NA 2 8 NA NA NA 2 1.5 222 0.5 218 NA NA NA NA NA NA 2 9 NA NA NA 2 1 517 11 517 NA NA NA NA NA NA 3 4 NA NA NA 2 22 1588 11 1596 NA NA NA NA NA NA 3 6 NA NA NA 2 0.5 150 4.5 306 0.5 152 NA NA NA NA 3 6 11 NA NA 3 12 868 5 857 NA NA NA NA NA NA 3 7 NA NA NA 2 16 1564 27 1584 NA NA NA NA NA NA 3 8 NA NA NA 2 3 228 3 225 NA NA NA NA NA NA 3 10 NA NA NA 2 9 173 4 176 NA NA NA NA NA NA 3 11 NA NA NA 2 6 336 5 334 NA NA NA NA NA NA 3 11 NA NA NA 2 END INITS #chain 1 list(sd.sq=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2,1,3,1, 1,1,0,-1), d = structure(.Data = c( NA,0,0,0,0,0,0,0,0,0,0, NA,NA,0,0,0,0,0,0,0,0,0, NA,NA,NA,0,0,0,0,0,0,0,0, NA,NA,NA,NA,0,0,0,0,0,0,0, NA,NA,NA,NA,NA,0,0,0,0,0,0, NA,NA,NA,NA,NA,NA,0,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,0,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,0,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,0,0, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,0 ), .Dim = c(10,11)) ) # chain 2 list(sd.sq=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0,1,3,1, 1,2,0,0), d = structure(.Data = c( NA,5,5,5,5,5,5,5,5,5,5, NA,NA,5,5,5,5,5,5,5,5,5, NA,NA,NA,5,5,5,5,5,5,5,5, NA,NA,NA,NA,5,5,5,5,5,5,5, NA,NA,NA,NA,NA,5,5,5,5,5,5, NA,NA,NA,NA,NA,NA,5,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,5,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,5,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,5,5, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,5 ), .Dim = c(10,11)) ) # chain 3 list(sd.sq=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1,1,3,1, 0,1,-1,-3), d = structure(.Data = c( NA,-3,-3,-3,-3,-3,-3,-3,-3,-3,3, NA,NA,-3,-3,-3,-3,-3,-3,-3,-3,3, NA,NA,NA,-3,-3,-3,-3,-3,-3,-3,3, NA,NA,NA,NA,-3,-3,-3,-3,-3,-3,3, NA,NA,NA,NA,NA,-3,-3,-3,-3,-3,3, NA,NA,NA,NA,NA,NA,-3,-3,-3,-3,3, NA,NA,NA,NA,NA,NA,NA,-3,-3,-3,3, NA,NA,NA,NA,NA,NA,NA,NA,-3,-3,3, NA,NA,NA,NA,NA,NA,NA,NA,NA,-3,-3, NA,NA,NA,NA,NA,NA,NA,NA,NA,NA,-3 ), .Dim = c(10,11)) )
M.3. Network meta-analysis for VTE prophylaxis in those undergoing abdominal surgery
M.3.1. Introduction
The results of conventional meta-analyses of direct evidence alone (as presented in the GRADE profiles in Chapter 35 and forest plots in appendix L) does not help inform which intervention is most effective as VTE prophylaxis in patients undergoing abdominal surgery. The challenge of interpretation has arisen for two reasons:
- In isolation, each pair-wise comparison does not inform the choice among the different treatments; in addition direct evidence is not available for some pair-wise comparisons in a randomised controlled trial.
- There are frequently multiple overlapping comparisons, which could potentially give inconsistent estimates of effect.
To overcome these problems, a hierarchical Bayesian network meta-analysis (NMA) was performed. This type of analysis allows for the synthesis of data from direct and indirect comparisons without breaking randomisation and allows for the ranking of different interventions. In this case the outcomes were defined as:
- Deep vein thrombosis (DVT; symptomatic and asymptomatic)
- Major bleeding
The analysis also provided estimates of effect (with 95% credible intervals) for each intervention compared to one another and compared to a single baseline risk (in this case the baseline treatment was no prophylaxis or in the case of the major bleeding outcome a combination of no prophylaxis and mechanical prophylaxis). These estimates provide a useful clinical summary of the results and facilitate the formation of recommendations based on the best available evidence.
Conventional fixed effects meta-analysis assumes that the relative effect of one treatment compared to another is the same across an entire set of trials. In a random effects model, it is assumed that the relative effects are different in each trial but that they are from a single common distribution and that this distribution is common across all sets of trials.
Network meta-analysis requires an additional assumption over conventional meta-analysis. The additional assumption is that intervention A has the same effect on people in trials of intervention A compared to intervention B as it does for people in trials of intervention A versus intervention C, and so on. Thus, in a random effects network meta-analysis, the assumption is that intervention A has the same effect distribution across trials of A versus B, A versus C and so on.
This specific method is usually referred to as mixed-treatment comparisons analysis but we will continue to use the term network meta-analysis to refer generically to this kind of analysis. We do so since the term “network” better describes the data structure, whereas “mixed treatments” could easily be misinterpreted as referring to combinations of treatments.
M.3.2. Methods
M.3.2.1. Study selection
To estimate the relative risks, we performed an NMA that simultaneously used all the relevant RCT evidence from the clinical evidence review. As with conventional meta-analyses, this type of analysis does not break the randomisation of the evidence, nor does it make any assumptions about adding the effects of different interventions. The effectiveness of a particular treatment strategy combination will be derived only from randomised controlled trials that had that particular combination in a trial arm.
M.3.2.2. Outcome measures
The NMA evidence reviews for interventions considered three clinical efficacy outcomes identified from the clinical evidence review; number of people with DVT, number of people with PE and number of people with major bleeding. Other outcomes were not considered for the NMA as they were infrequently reported across the studies. The committee considered that these outcomes were the most critical clinical outcomes for testing effectiveness of VTE prophylaxis.
M.3.2.3. Comparability of interventions
The interventions compared in the model were those found in the randomised controlled trials and included in the clinical evidence review already presented in Chapter 35 of the full guideline and in appendix H. If an intervention was evaluated in a study that met the inclusion criteria for the network (that is if it reported at least one of the outcomes of interest and matched the inclusion criteria for the meta-analysis) then it was included in the network meta-analysis, otherwise it was excluded.
The treatments included in each network are shown in Table 257.
Table 257Treatments included in network meta-analysis
|
Network 1: Number of people with DVT |
Network 2: Number of people with PE |
Network 3: Number of people with major bleeding. |
|---|---|---|
| Electrical stimulation | Fondaparinux standard duration | Fondaparinux standard duration |
| Fondaparinux standard duration | IPCD below knee | No/mechanical prophylaxis |
| Fondaparinux standard duration + IPCD any location | IPCD full leg | Post-operative LMWH standard duration, standard dose |
| Foot pump | No prophylaxis | Pre-operative LMWH extended duration, standard dose |
| IPCD below knee | Post-operative LMWH standard duration, standard dose | Pre-operative LMWH standard duration, high dose |
| IPCD full leg | Pre-operative LMWH extended duration, standard dose | Pre-operative LMWH standard duration, low dose |
| IPCD undefined | Pre-operative LMWH standard duration, low dose | Pre-operative LMWH standard duration, standard dose |
| No prophylaxis | Pre-operative LMWH standard duration, standard dose | UFH standard duration |
| Post-operative LMWH standard duration, standard dose | AES above knee | - |
| Post-operative LMWH standard duration, standard dose + IPCD undefined | AES above knee + IPCD full leg | - |
| Pre-operative LMWH extended duration, standard dose | AES above knee + UFH standard | - |
| Pre-operative LMWH standard duration, high dose | UFH standard duration | - |
| Pre-operative LMWH standard duration, low dose | VKA standard duration | - |
| Pre-operative LMWH standard duration, standard dose | - | - |
| AES above knee | - | - |
| AES above knee + IPCD full leg | - | - |
| AES above knee + UFH standard | - | - |
| AES below knee | - | - |
| AES combination + IPCD full leg | - | - |
| AES undefined | - | - |
| UFH standard duration | - | - |
| VKA standard duration | - | - |
The details of these interventions can be found in the clinical evidence review in Chapter 35 of the full guideline and evidence tables in appendix H.
M.3.2.4. Baseline risk
The baseline risk is defined here as the risk of achieving the outcome of interest in the no prophylaxis group. This figure is useful because it allows us to convert the results of the NMA from odds ratios to relative risks.
Baseline odds were derived by the logistic regression in WinBUGS. This approach has the advantage that baseline and relative effects are both modelled on the same log odds scale, and also ensures that the uncertainty in the estimation of baseline and relative effects is accounted for in the model. This method produced baseline odds [mean (SD)] as follows:
- −1.372 (1.174) for number of patients with DVT in the no prophylaxis group
- −3.939 (2.201) for number of patients with PE in the no prophylaxis group
- −5.331 (3.482) for the number of patients with major bleeding in the no/mechanical prophylaxis group.
For details of data informing these models, please refer to the full analyses in sections M.3.6.1, M.3.6.4 and M.3.6.6.
M.3.2.5. Statistical analysis
A hierarchical Bayesian network meta-analysis (NMA) was performed using the software WinBUGS. We adapted a three-arm random effects model template for the networks, from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). This model accounts for the correlation between study level effects induced by multi-arm trials.
In order to be included in the analysis, a fundamental requirement is that each treatment is connected directly or indirectly to every other intervention in the network. For each outcome subgroup, a diagram of the evidence network is presented in section M.3.3.
The model used was a random effects logistic regression model, with parameters estimated by Markov chain Monte Carlo simulation. As it was a Bayesian analysis, for each parameter the evidence distribution is weighted by a distribution of prior beliefs. These were estimated from the baseline models for the dichotomous outcomes using the following equations.
Predictive probability of response (MeanA) =mean of mu.new
Precision (PrecA)=1/(standard deviation of mu.new)2
A non-informative prior distribution was used to maximise the weighting given to the data for continuous outcomes. These priors were normally distributed with a mean of 0 and standard deviation of 10,000.
For the analyses, a series of 60,000 burn-in simulations were run to allow convergence and then a further 600,000 simulations were run to produce the outputs. For the baseline analyses, a series of 100,000 burn-in simulations were run to allow convergence and then a further 100,000 simulations were run to produce the outputs. Convergence was assessed by examining the history and kernel density plots.
We tested the goodness of fit of the model by calculating the residual deviance. If the residual deviance is close to the number of unconstrained data points (the number of trial arms in the analysis) then the model is explaining the data well.
The results, in terms of relative risk, of pair-wise meta-analyses are presented in the clinical evidence review (Chapter 35, and appendix H).
The aim of the NMA was to calculate treatment specific log odds ratios and relative risks for response to be consistent with the comparative effectiveness results presented elsewhere in the clinical evidence review and for ease of interpretation. Let BO, , and p denote the baseline odds, treatment specific odds, treatment specific log odds ratio and absolute probability respectively. Then:
And:
Once the treatment specific probabilities for response are calculated, we divide them by the baseline probability (pb) to get treatment specific relative risks (rrb):
This approach has the advantage that baseline and relative effects are both modelled on the same log odds scale, and also ensures that the uncertainty in the estimation of both baseline and relative effects is accounted for in the model.
We also calculated the overall ranking of interventions according to their relative risk compared to control group. Due to the skewness of the data, the NMA relative risks and rank results are reported as medians rather than means (as in the direct comparisons) to give a more accurate representation of the ‘most likely’ value. The median rank for each intervention was derived from the resulting distribution and these are presented on a rank plot with the associated 95% credible intervals.
A key assumption behind NMA is that the network is consistent. In other words, it is assumed that the direct and indirect treatment effect estimates do not disagree with one another. Discrepancies between direct and indirect estimates of effect may result from several possible causes. First, there is chance and if this is the case then the network meta-analysis results are likely to be more precise as they pool together more data than conventional meta-analysis estimates alone. Second, there could be differences between the trials included in terms of their clinical or methodological characteristics.
This heterogeneity is a problem for network meta-analysis but may be dealt with by subgroup analysis, meta-regression or by carefully defining inclusion criteria. Inconsistency, caused by heterogeneity, was assessed subjectively by comparing the relative risks from the direct evidence (from pair-wise meta-analysis) to the relative risks from the combined direct and indirect evidence (from NMA). We assumed the evidence to be inconsistent where the relative risk from the NMA did not fit within the confidence interval of the relative risk from the direct comparison. We further tested for inconsistency by developing inconsistency models for networks of binary outcomes using the TSD 4 template from the University of Bristol website (https://www.bris.ac.uk/cobm/research/mpes/mtc.html). We compared the posterior mean of the residual deviance between the consistency and inconsistency models to see which was a better fit to the data (closest to the number of trial arms in each network) and checked the difference in deviance information criterion (DIC) values between the two models was small (less than 3–5) or if it was larger, that the smaller DIC and hence better fitting model was the consistency model. No inconsistency was identified.
M.3.3. Results
M.3.3.1. Deep vein thrombosis (symptomatic and asymptomatic)
Included studies
66 studies were identified as reporting on DVT outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 48 studies involving 22 treatments were included in the network for DVT (symptomatic and asymptomatic). The network can be seen in Figure 839 and the trial data for each of the studies included in the NMA are presented in Table 258.

Figure 839Network diagram for DVT
Table 258Study data for DVT network meta-analysis
| Study | Intervention 1 | Intervention 2 | Intervention 3 | Intervention 1 | Intervention 2 | Intervention 3 | |||
|---|---|---|---|---|---|---|---|---|---|
| Events | N | Events | N | Events | N | ||||
| Coe 1978 | No prophylaxis | UFH standard | IPCD below knee | 6 | 24 | 6 | 28 | 2 | 29 |
| Tabemer 1978 | No prophylaxis | UFH standard | VKA standard | 11 | 48 | 3 | 49 | 3 | 48 |
| Bergqvist 1980 | No prophylaxis | UFH standard | NA | 14 | 51 | 6 | 46 | NA | NA |
| Clarke-Pearson 1983 | No prophylaxis | UFH standard | NA | 11 | 97 | 11 | 88 | NA | NA |
| Gallus 1973 | No prophylaxis | UFH standard | NA | 4 | 118 | 1 | 108 | NA | NA |
| Gallus 1976 | No prophylaxis | UFH standard | NA | 12 | 412 | 4 | 408 | NA | NA |
| Gordon-Smith 1972 | No prophylaxis | UFH standard | NA | 21 | 50 | 4 | 48 | NA | NA |
| Kakkar 1972 | No prophylaxis | UFH standard | NA | 17 | 39 | 3 | 39 | NA | NA |
| Strand 1925 | No prophylaxis | UFH standard | NA | 10 | 50 | 3 | 50 | NA | NA |
| Tomgren 1978 | No prophylaxis | UFH standard | NA | 20 | 61 | 10 | 63 | NA | NA |
| Vandendris 1980 | No prophylaxis | UFH standard | NA | 13 | 33 | 3 | 31 | NA | NA |
| Buston 1981 | No prophylaxis | IPCD below knee | NA | 4 | 57 | 6 | 62 | NA | NA |
| Clarke-Pearson 1984A | No prophylaxis | IPCD below knee | NA | 11 | 97 | 14 | 97 | NA | NA |
| Clarke-Pearson 1984B | No prophylaxis | IPCD below knee | NA | 17 | 52 | 5 | 55 | NA | NA |
| Allan 1983 | No prophylaxis | AES position not reported | NA | 37 | 103 | 15 | 97 | NA | NA |
| Tsapogas 1971 | No prophylaxis | AES below knee | NA | 6 | 44 | 2 | 51 | NA | NA |
| Halford 1976 | No prophylaxis | AES above knee | NA | 23 | 47 | 11 | 48 | NA | NA |
| Turner 1984 | No prophylaxis | AES above knee | NA | 4.5 | 93 | 0.5 | 105 | NA | NA |
| Scurr 1981 | No prophylaxis | Foot pump | NA | 15 | 33 | 6 | 33 | NA | NA |
| Marassi 1993 | No prophylaxis | Pre-operative LMWH standard high | NA | 11 | 31 | 2 | 30 | NA | NA |
| Bergqvist 1996 | No prophylaxis | Post-operative LMWH standard standard | NA | 9 | 41 | 3 | 39 | NA | NA |
| Ockelford 1989 | No prophylaxis | Pre-operative LMWH standard low | NA | 14 | 88 | 4 | 95 | NA | NA |
| Clarke-Pearson 1993 | UFH standard | IPCD below knee | NA | 6 | 107 | 3 | 101 | NA | NA |
| van Vroonhoven 1974 | UFH standard | VKA standard | NA | 1 | 50 | 9 | 50 | NA | NA |
| Leizorovicz 1991 | UFH standard | Pre-operative LMWH standard low | Pre-operative LMWH standard standard | 7 | 429 | 16 | 431 | 7 | 430 |
| Caen 1988 | UFH standard | Pre-operative LMWH standard low | NA | 7 | 190 | 6 | 195 | NA | NA |
| Hartl 1990 | UFH standard | Pre-operative LMWH standard low | NA | 5 | 115 | 5 | 112 | NA | NA |
| Koller 1986B | UFH standard | Pre-operative LMWH standard low | NA | 1 | 72 | 2 | 74 | NA | NA |
| Nurmohamed 1995 | UFH standard | Pre-operative LMWH standard low | NA | 8 | 709 | 25 | 718 | NA | NA |
| Bergqvist 1988 | UFH standard | Pre-operative LMWH standard standard | NA | 41 | 497 | 28 | 505 | NA | NA |
| Onarheim 1986 | UFH standard | Pre-operative LMWH standard standard | NA | 0.5 | 28 | 1.5 | 26 | NA | NA |
| Bergqvist 1986 | UFH standard | Pre-operative LMWH standard standard | NA | 9 | 217 | 13 | 215 | NA | NA |
| Wille-Jorgensen 1991 | UFH standard | AES above knee + UFH standard | NA | 12 | 81 | 2 | 79 | NA | NA |
| Wille-Jorgensen 1985 | UFH standard | AES above knee + UFH standard | NA | 7 | 90 | 1 | 86 | NA | NA |
| Nicolaides 1983 | UFH standard | Electrical stimulation | AES combination + IPCD full leg | 7 | 50 | 12 | 50 | 3 | 50 |
| Soderdahl 1997 | IPCD below knee | IPCD full leg | NA | 1.5 | 44 | 0.5 | 48 | NA | NA |
| Chandhoke 1992 | VKA standard | IPCD full leg | NA | 0.5 | 54 | 2.5 | 48 | NA | NA |
| Gao 2012 | AES position not reported | AES combination + IPCD full leg | NA | 14 | 56 | 5 | 52 | NA | NA |
| Porteous 1989 | AES below knee | AES above knee | NA | 1 | 58 | 3 | 56 | NA | NA |
| Caprini 1983 | AES above knee | AES above knee + IPCD full leg | NA | 5 | 39 | 1 | 38 | NA | NA |
| Harch 1988 | Pre-operative LMWH standard low | Pre-operative LMWH standard standard | NA | 2.5 | 17 | 0.5 | 20 | NA | NA |
| Bergqvist 1995 | Pre-operative LMWH standard low | Pre-operative LMWH standard standard | NA | 124 | 976 | 65 | 981 | NA | NA |
| Bergqvist 2002 | Pre-operative LMWH standard standard | Pre-operative LMWH extended standard | NA | 20 | 167 | 8 | 165 | NA | NA |
| Agnelli 2005 | Pre-operative LMWH standard standard | Fondaparinux standard | NA | 59 | 1018 | 43 | 1024 | NA | NA |
| Maxwell 2001 | Pre-operative LMWH standard standard | IPCD location un-defined | NA | 2 | 105 | 1 | 106 | NA | NA |
| Turpie 2007 | IPCD location un-defined | Fondaparinux standard + IPCD any location | NA | 22 | 418 | 7 | 424 | NA | NA |
| Sakon 2010 | IPCD location un-defined | IPCD undefined + Post-operative LMWH standard standard | NA | 6 | 31 | 1 | 78 | NA | NA |
| Song 2014 | IPCD location un-defined | IPCD undefined + Post-operative LMWH standard standard | NA | 3.5 | 113 | 0.5 | 109 | NA | NA |
NMA results
Table 259 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 259Risk ratios for DVT (symptomatic and asymptomatic)
| Comparisons | Risk ratio | ||
|---|---|---|---|
|
Direct (mean with 95% confidence interval) |
NMA (median with 95% credible interval) | ||
| Versus no prophylaxis | UFH standard | 0.36 (0.10, 1.27) | 0.35 (0.221, 0.62) |
| IPCD below knee | 0.64 (0.26, 1.59) | 0.53 (0.22, 0.95) | |
| VKA standard | 0.27 (0.08, 0.92) | 0.58 (0.17, 1.44) | |
| AES position not reported | 0.43 (0.25, 0.73) | 0.40 (0.12, 1.07) | |
| AES below knee | 0.29 (0.06, 1.35) | 0.18 (0.03, 0.82) | |
| AES above knee | 0.41 (0.23, 0.73) | 0.34 (0.10, 0.91) | |
| Foot pump | 0.40 (0.18, 0.90) | 0.32 (0.06, 1.20) | |
| Pre-operative LMWH standard duration, high dose | 0.19 (0.05, 0.78) | 0.14 (0.01, 0.83) | |
| Post-operative LMWH standard duration, standard dose | 0.35 (0.10, 1.20) | 0.34 (0.05, 1.41) | |
| Pre-operative LMWH standard duration, low dose | 0.26 (0.09, 0.77) | 0.57 (0.27, 1.01) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.31 (0.13, 0.69) | |
| AES above knee + UFH standard | - | 0.05 (0.01, 0.24) | |
| Electrical stimulation | - | 0.65 (0.15, 2.00) | |
| AES combination + IPCD full leg | - | 0.13 (0.03, 0.54) | |
| IPCD full leg | - | 0.85 (0.10, 3.90) | |
| AES above knee + IPCD full leg | - | 0.05 (0.00, 0.63) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.12 (0.02, 0.60) | |
| Fondaparinux standard | - | 0.23 (0.05, 0.87) | |
| IPCD location un-defined | - | 0.14 (0.00, 1.63) | |
| Fondaparinux standard + IPCD any location | - | 0.04 (0.00, 0.91) | |
| IPCD un-defined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.28) | |
| Versus UFH standard duration | IPCD below knee | 0.42 (0.16, 1.15) | 1.46 (0.72, 3.01) |
| VKA standard | 3.03 (1.00, 9.18) | 1.57 (0.53, 4.38) | |
| AES position not reported | - | 1.11 (0.34, 3.30) | |
| AES below knee | - | 0.52 (0.08, 2.44) | |
| AES above knee | - | 0.94 (0.27, 2.87) | |
| Foot pump | - | 0.89 (0.17, 3.80) | |
| Pre-operative LMWH standard duration, high dose | - | 0.40 (0.04, 2.43) | |
| Post-operative LMWH standard duration, standard dose | - | 0.93 (0.13, 4.49) | |
| Pre-operative LMWH standard duration, low dose | 1.27 (0.93, 1.73) | 1.57 (0.91, 2.76) | |
| Pre-operative LMWH standard duration, standard dose | 0.85 (0.59, 1.24) | 0.88 (0.46, 1.63) | |
| AES above knee + UFH standard | 0.16 (0.05, 0.54) | 0.14 (0.02, 0.57) | |
| Electrical stimulation | 1.71 (0.74, 3.99) | 1.75 (0.46, 6.06) | |
| AES combination + IPCD full leg | 0.43 (0.12, 1.56) | 0.38 (0.09, 1.38) | |
| IPCD full leg | - | 2.24 (0.30, 12.75) | |
| AES above knee + IPCD full leg | - | 0.13 (0.00, 1.76) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.34 (0.07, 1.52) | |
| Fondaparinux standard | - | 0.64 (0.16, 2.32) | |
| IPCD location un-defined | - | 0.38 (0.01, 4.66) | |
| Fondaparinux standard + IPCD any location | - | 0.11 (0.00, 2.43) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 0.74) | |
| Versus IPCD below knee | VKA standard | - | 1.09 (0.32, 3.45) |
| AES position not reported | - | 0.76 (0.21, 2.56) | |
| AES below knee | - | 0.36 (0.05, 1.79) | |
| AES above knee | - | 0.65 (0.17, 2.15) | |
| Foot pump | - | 0.61 (0.11, 2.80) | |
| Pre-operative LMWH standard duration, high dose | - | 0.28 (0.02, 1.76) | |
| Post-operative LMWH standard duration, standard dose | - | 0.64 (0.08, 3.27) | |
| Pre-operative LMWH standard duration, low dose | - | 1.07 (0.46, 2.60) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.60 (0.23, 1.52) | |
| AES above knee + UFH standard | - | 0.09 (0.01, 0.47) | |
| Electrical stimulation | - | 1.20 (0.27, 4.83) | |
| AES combination + IPCD full leg | - | 0.26 (0.05, 1.10) | |
| IPCD full leg | 0.31 (0.01, 7.31) | 1.54 (0.21, 8.61) | |
| AES above knee + IPCD full leg | - | 0.09 (0.00, 1.28) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.23 (0.04, 1.22) | |
| Fondaparinux standard | - | 0.44 (0.09, 1.88) | |
| IPCD location un-defined | - | 0.26 (0.01, 3.42) | |
| Fondaparinux standard + IPCD any location | - | 0.08 (0.00, 1.78) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.54) | |
| Versus VKA standard duration | AES position not reported | - | 0.71 (0.16, 3.10) |
| AES below knee | - | 0.33 (0.04, 2.08) | |
| AES above knee | - | 0.60 (0.13, 2.64) | |
| Foot pump | - | 0.56 (0.08, 3.25) | |
| Pre-operative LMWH standard duration, high dose | - | 0.26 (0.02, 2.01) | |
| Post-operative LMWH standard duration, standard dose | - | 0.59 (0.07, 3.77) | |
| Pre-operative LMWH standard duration, low dose | - | 0.99 (0.32, 3.34) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.56 (0.17, 1.93) | |
| AES above knee + UFH standard | - | 0.09 (0.01, 0.52) | |
| Electrical stimulation | - | 1.11 (0.21, 5.54) | |
| AES combination + IPCD full leg | - | 0.24 (0.04, 1.25) | |
| IPCD full leg | 0.18 (0.01, 3.60) | 1.41 (0.21, 8.02) | |
| AES above knee + IPCD full leg | - | 0.08 (0.00, 1.37) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.22 (0.03, 1.37) | |
| Fondaparinux standard | - | 0.41 (0.07, 2.14) | |
| IPCD location un-defined | - | 0.24 (0.01, 3.62) | |
| Fondaparinux standard + IPCD any location | - | 0.07 (0.00, 1.83) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.56) | |
| Versus AES position not reported | AES below knee | - | 0.47 (0.06, 3.03) |
| AES above knee | - | 0.85 (0.18, 3.87) | |
| Foot pump | - | 0.80 (0.12, 4.79) | |
| Pre-operative LMWH standard duration, high dose | - | 0.36 (0.03, 2.92) | |
| Post-operative LMWH standard duration, standard dose | - | 0.84 (0.10, 5.62) | |
| Pre-operative LMWH standard duration, low dose | - | 1.41 (0.44, 5.16) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.79 (0.22, 2.97) | |
| AES above knee + UFH standard | - | 0.12 (0.02, 0.77) | |
| Electrical stimulation | - | 1.57 (0.33, 7.46) | |
| AES combination + IPCD full leg | 0.38 (0.15, 0.99) | 0.34 (0.09, 1.17) | |
| IPCD full leg | - | 2.01 (0.22, 15.68) | |
| AES above knee + IPCD full leg | - | 0.12 (0.00, 1.97) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.31 (0.04, 2.06) | |
| Fondaparinux standard | - | 0.58 (0.10, 3.25) | |
| IPCD location un-defined | - | 0.34 (0.01, 5.60) | |
| Fondaparinux standard + IPCD any location | - | 0.10 (0.00, 2.73) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 0.81) | |
| Versus AES below the knee | AES above knee | 3.11 (0.33, 28.99) | 1.78 (0.37, 11.60) |
| Foot pump | - | 1.69 (0.19, 17.66) | |
| Pre-operative LMWH standard duration, high dose | - | 0.78 (0.05, 10.05) | |
| Post-operative LMWH standard duration, standard dose | - | 1.76 (0.16, 19.83) | |
| Pre-operative LMWH standard duration, low dose | - | 3.00 (0.61, 22.24) | |
| Pre-operative LMWH standard duration, standard dose | - | 1.68 (0.31, 12.43) | |
| AES above knee + UFH standard | - | 0.26 (0.02, 2.86) | |
| Electrical stimulation | - | 3.36 (0.45, 32.66) | |
| AES combination + IPCD full leg | - | 0.73 (0.09, 7.04) | |
| IPCD full leg | - | 4.27 (0.36, 54.64) | |
| AES above knee + IPCD full leg | - | 0.26 (0.01, 5.18) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.66 (0.07, 7.38) | |
| Fondaparinux standard | - | 1.23 (0.15, 12.30) | |
| IPCD location un-defined | - | 0.73 (0.02, 17.86) | |
| Fondaparinux standard + IPCD any location | - | 0.22 (0.00, 8.27) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.04 (0.00, 2.35) | |
| Versus AES above the knee | Foot pump | - | 0.94 (0.14, 5.77) |
| Pre-operative LMWH standard duration, high dose | - | 0.43 (0.03, 3.56) | |
| Post-operative LMWH standard duration, standard dose | - | 0.99 (0.12, 6.71) | |
| Pre-operative LMWH standard duration, low dose | - | 1.66 (0.51, 6.36) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.93 (0.26, 3.69) | |
| AES above knee + UFH standard | - | 0.15 (0.02, 0.96) | |
| Electrical stimulation | - | 1.86 (0.34, 10.48) | |
| AES combination + IPCD full leg | - | 0.40 (0.07, 2.30) | |
| IPCD full leg | - | 2.36 (0.26, 19.24) | |
| AES above knee + IPCD full leg | 0.21 (0.03, 1.68) | 0.15 (0.00, 1.43) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.36 (0.05, 2.50) | |
| Fondaparinux standard | - | 0.68 (0.11, 4.02) | |
| IPCD location un-defined | - | 0.41 (0.01, 6.71) | |
| Fondaparinux standard + IPCD any location | - | 0.12 (0.00, 3.29) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 0.98) | |
| Versus foot pump | Pre-operative LMWH standard duration, high dose | - | 0.46 (0.03, 4.87) |
| Post-operative LMWH standard duration, standard dose | - | 1.04 (0.10, 9.67) | |
| Pre-operative LMWH standard duration, low dose | - | 1.77 (0.39, 10.02) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.99 (0.20, 5.73) | |
| AES above knee + UFH standard | - | 0.16 (0.02, 1.36) | |
| Electrical stimulation | - | 1.97 (0.28, 15.29) | |
| AES combination + IPCD full leg | - | 0.43 (0.06, 3.34) | |
| IPCD full leg | - | 2.50 (0.23, 26.76) | |
| AES above knee + IPCD full leg | - | 0.15 (0.00, 3.09) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.39 (0.04, 3.56) | |
| Fondaparinux standard | - | 0.73 (0.09, 5.77) | |
| IPCD location un-defined | - | 0.43 (0.01, 8.79) | |
| Fondaparinux standard + IPCD any location | - | 0.13 (0.00, 4.15) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 1.19) | |
| Versus pre-operative LMWH standard duration, high dose | Post-operative LMWH standard duration, standard dose | - | 2.28 (0.17, 37.32) |
| Pre-operative LMWH standard duration, low dose | - | 3.89 (0.61, 44.72) | |
| Pre-operative LMWH standard duration, standard dose | - | 2.17 (0.32, 25.28) | |
| AES above knee + UFH standard | - | 0.34 (0.03, 5.45) | |
| Electrical stimulation | - | 4.36 (0.47, 63.35) | |
| AES combination + IPCD full leg | - | 0.94 (0.09, 13.53) | |
| IPCD full leg | - | 5.54 (0.41, 99.61) | |
| AES above knee + IPCD full leg | - | 0.33 (0.01, 10.68) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.85 (0.07, 13.89) | |
| Fondaparinux standard | - | 1.60 (0.16, 23.52) | |
| IPCD location un-defined | - | 0.95 (0.02, 30.24) | |
| Fondaparinux standard + IPCD any location | - | 0.28 (0.00, 13.34) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.05 (0.00, 3.76) | |
| Versus post-operative LMWH standard duration, standard dose | Pre-operative LMWH standard duration, low dose | - | 1.68 (0.33, 12.74) |
| Pre-operative LMWH standard duration, standard dose | - | 0.94 (0.17, 7.14) | |
| AES above knee + UFH standard | - | 0.15 (0.01, 1.61) | |
| Electrical stimulation | - | 1.88 (0.25, 18.67) | |
| AES combination + IPCD full leg | - | 0.41 (0.05, 4.02) | |
| IPCD full leg | - | 2.41 (0.20, 31.62) | |
| AES above knee + IPCD full leg | - | 0.15 (0.00, 3.45) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.37 (0.04, 4.13) | |
| Fondaparinux standard | - | 0.70 (0.08, 6.91) | |
| IPCD location un-defined | - | 0.42 (0.01, 9.72) | |
| Fondaparinux standard + IPCD any location | - | 0.12 (0.00, 4.59) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 1.28) | |
| Versus pre-operative LMWH standard duration, low dose | Pre-operative LMWH standard duration, standard dose | 0.51 (0.39, 0.66) | 0.56 (0.28, 1.05) |
| AES above knee + UFH standard | - | 0.09 (0.01, 0.41) | |
| Electrical stimulation | - | 1.13 (0.26, 4.17) | |
| AES combination + IPCD full leg | - | 0.24 (0.05, 0.98) | |
| IPCD full leg | - | 1.44 (0.18, 8.41) | |
| AES above knee + IPCD full leg | - | 0.08 (0.00, 1.19) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.22 (0.04, 0.98) | |
| Fondaparinux standard | - | 0.41 (0.10, 1.48) | |
| IPCD location un-defined | - | 0.24 (0.01, 2.94) | |
| Fondaparinux standard + IPCD any location | - | 0.07 (0.00, 1.54) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.48) | |
| Versus pre-operative LMWH standard duration, standard dose | AES above knee + UFH standard | - | 0.16 (0.02, 0.74) |
| Electrical stimulation | - | 1.99 (0.46, 8.11) | |
| AES combination + IPCD full leg | - | 0.43 (0.09, 1.82) | |
| IPCD full leg | - | 2.54 (0.32, 16.59) | |
| AES above knee + IPCD full leg | - | 0.15 (0.00, 2.19) | |
| Pre-operative LMWH extended duration, standard dose | 0.40 (0.18, 0.89) | 0.39 (0.09, 1.51) | |
| Fondaparinux standard | 0.72 (0.49, 1.06) | 0.73 (0.21, 2.28) | |
| IPCD location un-defined | 0.50 (0.05, 5.38) | 0.44 (0.01, 5.03) | |
| Fondaparinux standard + IPCD any location | - | 0.13 (0.00, 2.58) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.02 (0.00, 0.79) | |
| Versus AES above knee + UFH standard duration | Electrical stimulation | - | 12.82 (1.83, 112.70) |
| AES combination + IPCD full leg | - | 2.76 (0.37, 24.75) | |
| IPCD full leg | - | 16.32 (1.43, 199.70) | |
| AES above knee + IPCD full leg | - | 0.96 (0.02, 23.31) | |
| Pre-operative LMWH extended duration, standard dose | - | 2.49 (0.29, 24.71) | |
| Fondaparinux standard | - | 4.65 (0.65, 42.46) | |
| IPCD location un-defined | - | 2.76 (0.06, 62.80) | |
| Fondaparinux standard + IPCD any location | - | 0.83 (0.01, 28.66) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.16 (0.00, 8.15) | |
| Versus electrical stimulation | AES combination + IPCD full leg | - | 0.22 (0.04, 0.93) |
| IPCD full leg | - | 1.28 (0.13, 10.84) | |
| AES above knee + IPCD full leg | - | 0.08 (0.00, 1.38) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.20 (0.02, 1.40) | |
| Fondaparinux standard | - | 0.37 (0.06, 2.30) | |
| IPCD location un-defined | - | 0.22 (0.01, 3.67) | |
| Fondaparinux standard + IPCD any location | - | 0.06 (0.00, 1.83) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.55) | |
| Versus AES combination + IPCD full leg | IPCD full leg | - | 5.85 (0.58, 56.54) |
| AES above knee + IPCD full leg | - | 0.35 (0.01, 6.88) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.90 (0.11, 7.21) | |
| Fondaparinux standard | - | 1.69 (0.25, 11.55) | |
| IPCD location un-defined | - | 1.00 (0.02, 19.07) | |
| Fondaparinux standard + IPCD any location | - | 0.30 (0.01, 9.04) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.06 (0.00, 2.57) | |
| Versus IPCD full leg | AES above knee + IPCD full leg | - | 0.06 (0.00, 1.48) |
| Pre-operative LMWH extended duration, standard dose | - | 0.15 (0.01, 1.83) | |
| Fondaparinux standard | - | 0.29 (0.03, 2.98) | |
| IPCD location un-defined | - | 0.17 (0.00, 4.22) | |
| Fondaparinux standard + IPCD any location | - | 0.05 (0.00, 1.96) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.01 (0.00, 0.56) | |
| Versus AES above the knee + IPCD full leg | Pre-operative LMWH extended duration, standard dose | - | 2.61 (0.12, 143.30) |
| Fondaparinux standard | - | 4.88 (0.25, 260.40) | |
| IPCD location un-defined | - | 2.85 (0.04, 266.80) | |
| Fondaparinux standard + IPCD any location | - | 0.87 (0.01, 106.20) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.17 (0.00, 28.67) | |
| Versus pre-operative LMWH extended duration, standard dose | Fondaparinux standard | - | 1.88 (0.30, 12.20) |
| IPCD location un-defined | - | 1.11 (0.03, 19.99) | |
| Fondaparinux standard + IPCD any location | - | 0.33 (0.01, 9.53) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.06 (0.00, 2.69) | |
| Versus fondaparinux standard duration | IPCD location un-defined | - | 0.60 (0.02, 9.40) |
| Fondaparinux standard + IPCD any location | - | 0.18 (0.00, 4.57) | |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.03 (0.00, 1.31) | |
| Versus IPCD location un-defined | Fondaparinux standard + IPCD any location | 0.31 (0.14, 0.73) | 0.31 (0.07, 1.23) |
| IPCD undefined + Post-operative LMWH standard duration, standard dose | 0.09 (0.02, 0.46) | 0.06 (0.00, 0.42) | |
| Versus fondaparinux standard duration + IPCD any location | IPCD undefined + Post-operative LMWH standard duration, standard dose | - | 0.20 (0.01, 2.17) |
Figure 840 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 22 different interventions being evaluated in comparison with no prophylaxis.
.&p=BOOKS&id=561788_appmf14.jpg "Click on image to zoom")
Figure 840Rank order for interventions based the relative risk of experiencing DVT compared to baseline (no prophylaxis)
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
The random effects model used for the NMA is a relatively good fit, with a residual deviance of 101 reported. This corresponds fairly well to the total number of trial arms, 100. The between trial standard deviation in the random effects analysis was 0.57 (95% CI 0.23 to 0.96). On evaluating inconsistency by comparing risk ratios, the NMA estimated risk ratio for IPCD below the knee compared to UFH at a standard duration (1.46 [0.72, 3.01]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (0.42 [0.16, 1.15]). An inconsistency model was run and the DIC statistics were as follows in Table 260. The difference in the DIC is small (<3–5) with the consistency model having the lower DIC value. This suggests that it fits the data better than the inconsistency model.
Table 260DIC for DVT (symptomatic and asymptomatic) – random effects
| DIC | TotResDev | |
|---|---|---|
| Consistency model | 530.880 | 101 |
| Inconsistency model | 532.606 | 100 |
M.3.3.2. Pulmonary embolism (PE)
Included studies
51 studies were identified as reporting on PE outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 26 studies involving 13 treatments were included in the network for PE. The network can be seen in Figure 841 and the trial data for each of the studies included in the NMA are presented in Table 261.

Figure 841Network diagram for PE
Table 261Study data for PE network meta-analysis
| Study | Intervention 1 | Intervention 2 | Intervention 3 | Intervention 1 | Intervention 2 | Intervention 3 | |||
|---|---|---|---|---|---|---|---|---|---|
| Events | N | Events | N | Events | N | ||||
| Clarke-Pearson 1984A | no prophylaxis | IPCD below knee | NA | 1 | 97 | 4 | 97 | NA | NA |
| Clarke-Pearson 1984B | no prophylaxis | IPCD below knee | NA | 1 | 52 | 2 | 55 | NA | NA |
| Coe 1978 | no prophylaxis | IPCD below knee | UFH standard | 1 | 24 | 1 | 29 | 1 | 28 |
| Gordon-Smith 1972 | no prophylaxis | UFH standard | NA | 0.5 | 51 | 2.5 | 49 | NA | NA |
| Bejjani 1983 | no prophylaxis | UFH standard | NA | 1.5 | 18 | 0.5 | 18 | NA | NA |
| Clarke-Pearson 1983 | no prophylaxis | UFH standard | NA | 0.5 | 98 | 4.5 | 89 | NA | NA |
| Lahnborg 1975 + 1974 | no prophylaxis | UFH standard | NA | 24 | 54 | 9 | 58 | NA | NA |
| Tongren 1978 | no prophylaxis | UFH standard | NA | 2 | 61 | 1 | 63 | NA | NA |
| Bergqvist 1996 | no prophylaxis | Post op LMWH standard standard | NA | 1.5 | 42 | 0.5 | 40 | NA | NA |
| Ockelford 1989 | no prophylaxis | Pre op LMWH standard low | NA | 2.5 | 89 | 0.5 | 96 | NA | NA |
| Holford 1976 | no prophylaxis | AES above knee | NA | 1.5 | 48 | 0.5 | 49 | NA | NA |
| Soderdahl 1997 | IPCD below knee | IPCD full leg | NA | 0.5 | 44 | 1.5 | 48 | NA | NA |
| Borstad 1992 | UFH standard | Pre op LMWH standard low | NA | 0.5 | 71 | 1.5 | 72 | NA | NA |
| Caen 1988 | UFH standard | Pre op LMWH standard low | NA | 1.5 | 191 | 0.5 | 196 | NA | NA |
| Kakkar 1993 | UFH standard | Pre op LMWH standard low | NA | 11 | 1915 | 8 | 1894 | NA | NA |
| Koller 1986 | UFH standard | Pre op LMWH standard low | NA | 1.5 | 73 | 0.5 | 75 | NA | NA |
| Leizorovicz 1991 | UFH standard | Pre op LMWH standard low | Pre op LMWH standard standard | 2 | 429 | 4 | 431 | 1 | 430 |
| Wille-Jorgensen 1985 | UFH standard | AES above knee + UFH standard | NA | 6 | 90 | 2 | 86 | NA | NA |
| Bergqvist 1988 | UFH standard | Pre op LMWH standard standard | NA | 4.5 | 498 | 0.5 | 506 | NA | NA |
| Fricker 1988 | UFH standard | Pre op LMWH standard standard | NA | 5.5 | 41 | 0.5 | 41 | NA | NA |
| McLeod 2001 | UFH standard | Pre op LMWH standard standard | NA | 0.5 | 469 | 1.5 | 469 | NA | NA |
| Bergqvist 1995 | Pre op LMWH standard low | Pre op LMWH standard standard | NA | 4 | 976 | 6 | 981 | NA | NA |
| Caprini 1983 | AES above knee | AES above knee + IPCD full leg | NA | 1 | 39 | 1 | 38 | NA | NA |
| Chandhoke 1992 | IPCD full leg | VKA standard | NA | 1.5 | 48 | 0.5 | 54 | NA | NA |
| Bergqvist 2002 | Pre op LMWH standard standard | Pre op LMWH extended standard | NA | 2.5 | 168 | 0.5 | 166 | NA | NA |
| Agnelli 2005 | Pre op LMWH standard standard | Fondaparinux standard | NA | 0.5 | 1463 | 2.5 | 1466 | NA | NA |
NMA results
Table 262 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 262Risk ratios for PE
| Comparisons | Risk ratio | ||
|---|---|---|---|
|
Direct (mean with 95% confidence interval) |
NMA (median with 95% credible interval) | ||
| Versus no prophylaxis | IPCD below the knee | 2.19 (0.58, 8.24) | 1.87 (0.34, 11.08) |
| UFH standard duration | 0.60 (0.36, (1.02) | 0.81 (0.26, 2.75) | |
| Post-operative LMWH standard duration, standard dose | 0.35 (0.01, 8.34) | 0.20 (0.00, 8.38) | |
| Pre-operative LMWH standard duration, low dose | 0.19 (0.01, 3.81) | 0.50 (0.10, 2.32) | |
| AES above the knee | 0.33 (0.01, 7.82) | 0.20 (0.00, 8.23) | |
| IPCD full leg | - | 5.32 (0.12, 238.70) | |
| AES above knee + UFH standard duration | - | 0.24 (0.01, 4.41) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.29 (0.04, 1.70) | |
| AES above the knee + IPCD full leg | - | 0.19 (0.00, 27.36) | |
| VKA standard duration | - | 1.40 (0.00, 160.60) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.03 (0.00, 1.84) | |
| Fondaparinux standard duration | - | 2.20 (0.04, 136.90) | |
| Versus IPCD below the knee | UFH standard duration | 1.04 (0.06, 17.00) | 0.43 (0.06, 3.17) |
| Post-operative LMWH standard duration, standard dose | - | 0.10 (0.00, 6.18) | |
| Pre-operative LMWH standard duration, low dose | - | 0.26 (0.03, 2.39) | |
| AES above the knee | - | 0.10 (0.00, 6.02) | |
| IPCD full leg | 2.75 (0.12, 65.76) | 2.61 (0.09, 113.50) | |
| AES above knee + UFH standard duration | - | 0.13 (0.00, 3.39) | |
| Pre-operative LMWH standard duration, standard dose | - | 0.15 (0.01, 1.63) | |
| AES above the knee + IPCD full leg | - | 0.10 (0.00, 18.30) | |
| VKA standard duration | - | 0.81 (0.00, 74.14) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.01 (0.00, 1.31) | |
| Fondaparinux standard duration | - | 1.21 (0.01, 93.75) | |
| Versus UFH standard duration | Post-operative LMWH standard duration, standard dose | - | 0.24 (0.00, 12.32) |
| Pre-operative LMWH standard duration, low dose | 0.88 (0.44, 1.78) | 0.62 (0.17, 1.88) | |
| AES above the knee | - | 0.24 (0.00, 12.26) | |
| IPCD full leg | - | 6.53 (0.13, 348.10) | |
| AES above knee + UFH standard duration | 0.35 (0.07, 1.68) | 0.31 (0.01, 3.98) | |
| Pre-operative LMWH standard duration, standard dose | 0.24 (0.06, 0.93) | 0.37 (0.07, 1.35) | |
| AES above the knee + IPCD full leg | - | 0.24 (0.00, 39.87) | |
| VKA standard duration | - | 1.66 (0.00, 226.70) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.04 (0.00, 1.85) | |
| Fondaparinux standard duration | - | 2.63 (0.05, 167.50) | |
| Versus post-operative LMWH standard duration, standard dose | Pre-operative LMWH standard duration, low dose | - | 2.59 (0.04, 2169.00) |
| AES above the knee | - | 1.01 (0.00, 1859.00) | |
| IPCD full leg | - | 30.87 (0.14, 52120.00) | |
| AES above knee + UFH standard duration | - | 1.31 (0.01, 1562.00) | |
| Pre-operative LMWH standard duration, standard dose | - | 1.54 (0.02, 1365.00) | |
| AES above the knee + IPCD full leg | - | 1.06 (0.00, 3598.00) | |
| VKA standard duration | - | 6.91 (0.00, 20470.00) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.16 (0.00, 316.50) | |
| Fondaparinux standard duration | - | 12.75 (0.04, 23960.00) | |
| Versus pre-operative LMWH standard duration, low dose | AES above the knee | - | 0.40 (0.00, 24.51) |
| IPCD full leg | - | 10.89 (0.19, 678.30) | |
| AES above knee + UFH standard duration | - | 0.50 (0.02, 9.11) | |
| Pre-operative LMWH standard duration, standard dose | 0.87 (0.32, 2.40) | 0.60 (0.12, 2.60) | |
| AES above the knee + IPCD full leg | - | 0.39 (0.00, 77.56) | |
| VKA standard duration | - | 2.60 (0.00, 435.90) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.06 (0.00, 3.30) | |
| Fondaparinux standard duration | - | 4.27 (0.09, 313.00) | |
| Versus AES above the knee | IPCD full leg | - | 31.09 (0.14, 43070.00) |
| AES above knee + UFH standard duration | - | 1.28 (0.01, 1369.00) | |
| Pre-operative LMWH standard duration, standard dose | - | 1.49 (0.02, 1131.00) | |
| AES above the knee + IPCD full leg | 1.03 (0.07, 15.82) | 1.05 (0.02. 45.55) | |
| VKA standard duration | - | 6.81 (0.00, 18380.00) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.16 (0.00, 279.10) | |
| Fondaparinux standard duration | - | 12.43 (0.05, 21680.00) | |
| Versus IPCD full leg | AES above knee + UFH standard duration | - | 0.04 (0.00, 4.81) |
| Pre-operative LMWH standard duration, standard dose | - | 0.05 (0.00, 3.41) | |
| AES above the knee + IPCD full leg | - | 0.03 (0.00, 16.57) | |
| VKA standard duration | 0.30 (0.01, 7.10) | 0.30 (0.00, 4.49) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.00 (0.00, 1.35) | |
| Fondaparinux standard duration | - | 0.50 (0.00, 101.50) | |
| Versus AES above the knee + UFH standard duration | Pre-operative LMWH standard duration, standard dose | - | 1.20 (0.06, 31.58) |
| AES above the knee + IPCD full leg | - | 0.78 (0.00, 316.10) | |
| VKA standard duration | - | 5.00 (0.00, 1871.00) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.12 (0.00, 17.72) | |
| Fondaparinux standard duration | - | 8.99 (0.09, 1518.00) | |
| Versus pre-operative LMWH standard duration, standard dose | AES above the knee + IPCD full leg | - | 0.65 (0.00, 147.90) |
| VKA standard duration | - | 4.32 (0.00, 830.30) | |
| Pre-operative LMWH extended duration, standard dose | 0.20 (0.01, 4.18) | 0.11 (0.00, 4.23) | |
| Fondaparinux standard duration | 4.99 (0.24, 103.84) | 6.99 (0.22, 484.90) | |
| Versus AES above the knee + IPCD full leg | VKA standard duration | - | 6.39 (0.00, 46310.00) |
| Pre-operative LMWH extended duration, standard dose | - | 0.15 (0.00, 724.50) | |
| Fondaparinux standard duration | - | 12.24 (0.02, 57240.00) | |
| Versus VKA standard duration | Pre-operative LMWH extended duration, standard dose | - | 0.02 (0.00, 121.10) |
| Fondaparinux standard duration | - | 1.55 (0.00, 9161.00) | |
| Versus pre-operative LMWH extended duration, standard dose | Fondaparinux standard duration | - | 80.07 (0.41, 134600.00) |
Figure 842 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 13 different interventions being evaluated.
.&p=BOOKS&id=561788_appmf16.jpg "Click on image to zoom")
Figure 842Rank order for interventions based the relative risk of experiencing PE compared to baseline (no prophylaxis)
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration; ed = extended duration
Goodness of fit and inconsistency
The random effects model used for the NMA is a relatively good fit, with a residual deviance of 55 reported. This corresponds well to the total number of trial arms, 54. The between trial standard deviation in the random effects analysis was 1.01 (95% CI 0.30 to 2.11). No inconsistency was identified between the direct RR and NMA results. An inconsistency model was run and the DIC statistics were as follows in Table 263. The difference in the DIC is small (<3–5) with the consistency model having the lower DIC value. This suggests that it fits the data better than the inconsistency model.
Table 263DIC for PE – random effects
| DIC | TotResDev | |
|---|---|---|
| Consistency model | 224.072 | 55 |
| Inconsistency model | 225.681 | 56 |
M.3.3.3. Major bleeding
Included studies
33 studies were identified as reporting on major bleeding outcomes. After excluding papers that reported zero events in each arm and papers reporting on combinations that did not connect to any other intervention in the network, 29 studies involving 8 treatments were included in the network for major bleeding. The network can be seen in Figure 843 and the trial data for each of the studies included in the NMA are presented in Table 264.

Figure 843Network diagram for major bleeding
Table 264Study data for major bleeding network meta-analysis
| Study | Intervention 1 | Intervention 2 | Intervention 3 | Intervention 1 | Intervention 2 | Intervention 3 | |||
|---|---|---|---|---|---|---|---|---|---|
| Events | N | Events | N | Events | N | ||||
| Ockelford 1989 | no prophylaxis/mechanical | pre op LMWH standard duration, low dose | NA | 4 | 88 | 4 | 95 | NA | NA |
| Osman 2007 | no prophylaxis/mechanical | UFH standard duration | Post op LMWH standard duration, standard dose | 0 | 25 | 0 | 25 | 1 | 25 |
| Allen 1978 | no prophylaxis/mechanical | UFH standard duration | NA | 0 | 30 | 6 | 30 | NA | NA |
| Bejjani 1983 | no prophylaxis/mechanical | UFH standard duration | NA | 0 | 17 | 1 | 17 | NA | NA |
| Tongren 1978 | no prophylaxis/mechanical | UFH standard duration | NA | 23 | 61 | 24 | 63 | NA | NA |
| Bergqvist 1996 | no prophylaxis/mechanical | Post op LMWH standard duration, standard dose | NA | 0 | 41 | 1 | 39 | NA | NA |
| Nagata 2015 | no prophylaxis/mechanical | Post op LMWH standard duration, standard dose | NA | 1 | 14 | 2 | 16 | NA | NA |
| Sakon 2010 | no prophylaxis/mechanical | Post op LMWH standard duration, standard dose | NA | 1 | 38 | 5 | 109 | NA | NA |
| Song 2014 | no prophylaxis/mechanical | Post op LMWH standard duration, standard dose | NA | 0 | 112 | 2 | 108 | NA | NA |
| Turpie 2007 | no prophylaxis/mechanical | Fondaparinux standard duration | NA | 1 | 650 | 10 | 635 | NA | NA |
| Borstad 1992 | pre op LMWH standard duration, low dose | UFH standard duration | NA | 14 | 71 | 9 | 70 | NA | NA |
| Kaaja 1992 | pre op LMWH standard duration, low dose | UFH standard duration | NA | 0 | 37 | 6 | 31 | NA | NA |
| Kakkar 1993 | pre op LMWH standard duration, low dose | UFH standard duration | NA | 69 | 1894 | 91 | 1915 | NA | NA |
| Koller 1986B | pre op LMWH standard duration, low dose | UFH standard duration | NA | 17 | 74 | 23 | 72 | NA | NA |
| Leizorovicz 1991 | pre op LMWH standard duration, low dose | UFH standard duration | pre op LMWH standard duration, standard dose | 14 | 431 | 12 | 429 | 10 | 430 |
| Hartl 1990 | pre op LMWH standard duration, low dose | UFH standard duration | NA | 2 | 112 | 15 | 115 | NA | NA |
| Nurmohamed 1995 | pre op LMWH standard duration, low dose | UFH standard duration | NA | 11 | 725 | 18 | 719 | NA | NA |
| Bergqvist 1995 | pre op LMWH standard duration, low dose | pre op LMWH standard duration, standard dose | NA | 3 | 1034 | 13 | 1036 | NA | NA |
| Hauch 1988 | pre op LMWH standard duration, low dose | pre op LMWH standard duration, standard dose | NA | 0 | 16 | 1 | 19 | NA | NA |
| Bergqvist 1986 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 2 | 217 | 10 | 215 | NA | NA |
| Borstad 1988 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 13 | 110 | 32 | 105 | NA | NA |
| Fricker 1988 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 1 | 40 | 2 | 40 | NA | NA |
| Gonzalez 1996 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 5 | 82 | 0 | 84 | NA | NA |
| McLeod 2001 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 10 | 643 | 18 | 653 | NA | NA |
| Onarheim 1986 | UFH standard duration | pre op LMWH standard duration, standard dose | NA | 1 | 27 | 1 | 25 | NA | NA |
| Koller 1986 A | UFH standard duration | pre op LMWH standard duration, high dose | NA | 1 | 20 | 6 | 23 | NA | NA |
| Agnelli 2005 | Fondaparinux standard duration | pre op LMWH standard duration, standard dose | NA | 49 | 1433 | 34 | 1425 | NA | NA |
| Bergqvist 2002 | pre op LMWH standard duration, standard dose | pre op LMWH extended duration, standard dose | NA | 1 | 248 | 3 | 253 | NA | NA |
| Rasmussen 2006 | pre op LMWH standard duration, standard dose | pre op LMWH extended duration, standard dose | NA | 4 | 222 | 1 | 205 | NA | NA |
NMA results
Table 265 summarises the results of the conventional meta-analyses in terms of risk ratios generated from studies directly comparing different interventions, together with the results of the NMA in terms of risk ratios for every possible treatment comparison.
Table 265Risk ratios for major bleeding
| Comparisons | Risk ratio | ||
|---|---|---|---|
|
Direct (mean with 95% confidence interval) |
NMA (median with 95% credible interval) | ||
| Versus no prophylaxis (or mechanical prophylaxis) | Pre-operative LMWH standard duration, low dose | 0.93 (0.24, 3.59) | 1.21 (0.41, 3.95) |
| UFH standard duration | 1.30 (0.84, 2.00) | 2.01 (0.81, 6.52) | |
| Post-operative LMWH standard duration, standard dose | 2.49 (0.78, 7.91) | 2.98 (0.88, 14.80) | |
| Fondaparinux standard duration | 10.24 (1.31, 79.73) | 4.98 (1.05, 31.16) | |
| Pre-operative LMWH standard duration, standard dose | - | 2.96 (1.00, 11.16) | |
| Pre-operative LMWH standard duration, high dose | - | 11.26 (1.02, 349.30) | |
| Pre-operative LMWH extended duration, standard dose | - | 2.39 (0.32, 22.51) | |
| Versus pre-operative LMWH standard duration, low dose | UFH standard duration | 1.36 (0.9, 2.05) | 1.64 (0.94, 3.53) |
| Post-operative LMWH standard duration, standard dose | - | 2.35 (0.50, 16.10) | |
| Fondaparinux standard duration | - | 4.01 (1.00, 24.20) | |
| Pre-operative LMWH standard duration, standard dose | 1.73 (0.42, 7.19) | 2.41 (1.02, 6.33) | |
| Pre-operative LMWH standard duration, high dose | - | 8.95 (0.99, 265.00) | |
| Pre-operative LMWH extended duration, standard dose | - | 1.92 (0.29, 15.24) | |
| Versus UFH standard duration | Post-operative LMWH standard duration, standard dose | 0.33 (0.01, 7.81) | 1.40 (0.31, 8.28) |
| Fondaparinux standard duration | - | 2.36 (0.62, 12.34) | |
| Pre-operative LMWH standard duration, standard dose | 1.67 (1.17, 2.39) | 1.43 (0.74, 3.04) | |
| Pre-operative LMWH standard duration, high dose | 5.22 (0.68, 39.74) | 5.17 (0.64, 138.20) | |
| Pre-operative LMWH extended duration, standard dose | - | 1.18 (0.17, 7.89) | |
| Versus post-operative LMWH standard duration, standard dose | Fondaparinux standard duration | - | 1.50 (0.24, 13.47) |
| Pre-operative LMWH standard duration, standard dose | - | 0.99 (0.17, 5.35) | |
| Pre-operative LMWH standard duration, high dose | - | 3.32 (0.26, 122.30) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.89 (0.07, 8.93) | |
| Versus fondaparinux standard duration | Pre-operative LMWH standard duration, standard dose | 0.70 (0.45, 1.07) | 0.63 (0.13, 2.18) |
| Pre-operative LMWH standard duration, high dose | - | 1.96 (0.16, 65.24) | |
| Pre-operative LMWH extended duration, standard dose | - | 0.55 (0.05, 4.00) | |
| Versus pre-operative LMWH standard duration, standard dose | Pre-operative LMWH standard duration, high dose | - | 3.46 (0.39, 97.05) |
| Pre-operative LMWH extended duration, standard dose | 0.83 (0.22, 3.12) | 0.90 (0.13, 4.66) | |
| Versus pre-operative LMWH standard duration, high dose | Pre-operative LMWH extended duration, standard dose | - | 0.25 (0.01, 3.49) |
Figure 844 shows the rank of each intervention compared to the others. The rank is based on the relative risk compared to baseline and indicates the probability of being the best treatment, second best, third best and so on among the 8 different interventions being evaluated.
.&p=BOOKS&id=561788_appmf18.jpg "Click on image to zoom")
Figure 844Rank order for interventions based the relative risk of major bleeding compared to baseline (no prophylaxis/mechanical prophylaxis)
LD = low dose; SD = standard dose; HD = high dose; sd = standard duration
Goodness of fit and inconsistency
The random effects model used for the NMA is a relatively good fit, with a residual deviance of 59 reported. This corresponds fairly well to the total number of trial arms, 60. The between trial standard deviation in the random effects analysis was 0.82 (95% CI 0.40 to 1.44). On evaluating inconsistency by comparing risk ratios, the NMA estimated risk ratio for UFH at a standard duration compared to no prophylaxis (2.01 [0.81, 6.52]) lay outside of the confidence interval of the risk ratio estimated for the direct comparison (1.30 [0.84, 2.00]). Therefore an inconsistency model was run and the DIC statistics were as follows in Table 266. The difference in the DIC is small (<3–5) which suggests that there is no obvious inconsistency in the network.
Table 266DIC for major bleeding – random effects
| DIC | TotResDev | |
|---|---|---|
| Consistency model | 299.227 | 59 |
| Inconsistency model | 302.084 | 60 |
M.3.4. Discussion
Based on the results of conventional meta-analyses of direct evidence, as has been previously presented in Chapter 35 and appendix H, deciding upon the most clinical and cost effective prophylaxis intervention in patients undergoing abdominal surgery is challenging. In order to overcome the difficulty of interpreting the conclusions from numerous separate comparisons, network meta-analysis of the direct evidence was performed. The findings of the NMA were used to facilitate the committee in decision-making when developing recommendations.
Our analyses were divided into three critical outcomes. 48 studies informed the DVT network where 22 different individual or combination treatments were evaluated including 10 mechanical interventions, eight pharmacological interventions, and three interventions that combined both mechanical and pharmacological prophylaxis. 26 studies informed the PE network of 13 different treatments, including four mechanical interventions, seven pharmacological interventions, and one intervention that combined both mechanical and pharmacological prophylaxis. The major bleeding network included 29 studies evaluating eight treatments, seven of which were pharmacological as for this outcome any mechanical prophylaxis measures were combined with the no prophylaxis intervention as it is believed that mechanical prophylaxis has no associated bleeding risk.
In the DVT network, the three interventions that represented a combination of mechanical and pharmacological prophylaxis featured in the top four best ranked treatments. IPCD (undefined location) plus post-operative LMWH at a standard duration and standard dose was ranked first, IPCD (any location) plus fondaparinux for a standard duration was ranked second, and AES above the knee plus unfractionated heparin for a standard duration was ranked fourth. The treatment in the third spot was a combination of two forms of mechanical prophylaxis (AES above the knee plus IPCD full leg). There is considerable uncertainty about these estimates as the credible intervals are quite wide (with the top intervention spanning nine ranking positions, and the second and third spanning 19 and 18 respectively).
In the PE network the only combination intervention evaluated (AES above the knee plus unfractionated heparin standard duration) came in fifth, and was outranked by pre-operative LMWH extended duration and standard dose, AES above the knee plus IPCD full leg, post-operative LMWH standard duration and standard dose, and AES above the knee alone. However the credible intervals were very wide, with the top ranked treatment spanning 10 rankings, the second and third treatments spanning all 13 rankings, and the fourth and fifth treatments spanning 12 rankings.
In the major bleeding network the highest ranked intervention was no prophylaxis/mechanical prophylaxis. This was followed by the low dose of pre-operative LMWH for a standard duration (with a credible interval spanning four ranking positions). This was followed by unfractionated heparin for a standard duration, then the three standard doses of LMWH preoperatively for either an extended or standard duration, or post-operatively for a standard duration. Fondaparinux for a standard duration came in seventh, and last was the high dose of pre-operative LMWH for a standard duration.
In summary, the three outcomes chosen for analyses were considered to be among the most critical for assessing clinical effectiveness of different VTE prophylaxis strategies. All three networks seemed to fit well, as demonstrated by residual deviance and no obvious inconsistency found in the networks. However the credible intervals around the ranking of treatments in all three networks were wide suggesting considerable uncertainty about these results.
M.3.5. Conclusion
This analysis allowed us to combine findings from many different comparisons presented in the review even when direct comparative data was lacking.
Overall the committee agreed that the results for the three networks were not conclusive. It was acknowledged that a combination of mechanical and pharmacological prophylaxis were likely to be the most effective prophylaxis and therefore may be appropriate to offer those people undergoing abdominal surgery who have been assessed as having a low risk of bleeding. For details of the rationale and discussion leading to recommendations, please refer to the section linking the evidence to the recommendations (section 35.6, chapter 35).
M.3.6. WinBUGS code
M.3.6.1. WinBUGS code for assessment of baseline risk of DVT
# Binomial likelihood, logit link # Baseline random effects model model{ # *** PROGRAM STARTS for (i in 1:ns){ # LOOP THROUGH STUDIES r[i] ~ dbin(p[i],n[i]) # Likelihood logit(p[i]) <- mu[i] # Log-odds of response mu[i] ~ dnorm(m,tau.m) # Random effects model } mu.new ~ dnorm(m,tau.m) # predictive dist. (log-odds) m ~ dnorm(0,.0001) # vague prior for mean var.m <- 1/tau.m # between-trial variance tau.m <- pow(sd.m,-2) # between-trial precision = (1/between-trial variance) sd.m ~ dunif(0,5) # vague prior for between-trial SD #tau.m ~ dgamma(0.001,0.001) #sd.m <- sqrt(var.m) logit(R) <- m # posterior probability of response logit(R.new) <- mu.new # predictive probability of response } Data list(ns=22) # ns=number of studies r[] n[] 6 24 11 48 14 51 11 97 4 118 12 412 21 50 17 39 10 50 20 61 13 33 4 57 11 97 17 52 37 103 6 44 23 47 4 92 15 33 11 31 9 41 14 88 END Inits list(mu=c(0,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0), sd.m=1, m=0) list(mu = c(-1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1,-1), sd.m=2, m= -1) list(mu = c(1,1,1,1,1, 1,1,1,1,1, 1,1,1,1,1, 1,1,1,1,1, 1,1), sd.m = 0.5, m = 1)
M.3.6.2. WinBUGS code for number of patients with DVT
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
sd ~ dunif(0,5) # vague prior for random effects standard deviation
tau <- 1/pow(sd,2)
A ~ dnorm(meanA, precA) # A is on log-odds scale
precA <- pow(sdA,-2) # turn st dev into precision
for (k in 1:NT){ # v[1] will give prob of event on treat 1
logit(v[k]) <- A + d[k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NS=48, NT=22, meanA=-1.371, sdA=1.105)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
6 24 6 28 2 29 1 2 3 3
11 48 3 49 3 48 1 2 4 3
14 51 6 46 NA NA 1 2 NA 2
11 97 11 88 NA NA 1 2 NA 2
4 118 1 108 NA NA 1 2 NA 2
12 412 4 408 NA NA 1 2 NA 2
21 50 4 48 NA NA 1 2 NA 2
17 39 3 39 NA NA 1 2 NA 2
10 50 3 50 NA NA 1 2 NA 2
20 61 10 63 NA NA 1 2 NA 2
13 33 3 31 NA NA 1 2 NA 2
4 57 6 62 NA NA 1 3 NA 2
11 97 14 97 NA NA 1 3 NA 2
17 52 5 55 NA NA 1 3 NA 2
37 103 15 97 NA NA 1 5 NA 2
6 44 2 51 NA NA 1 6 NA 2
23 47 11 48 NA NA 1 7 NA 2
4.5 93 0.5 105 NA NA 1 7 NA 2
15 33 6 33 NA NA 1 8 NA 2
11 31 2 30 NA NA 1 9 NA 2
9 41 3 39 NA NA 1 10 NA 2
14 88 4 95 NA NA 1 11 NA 2
6 107 3 101 NA NA 2 3 NA 2
1 50 9 50 NA NA 2 4 NA 2
7 429 16 431 7 430 2 11 12 3
7 190 6 195 NA NA 2 11 NA 2
5 115 5 112 NA NA 2 11 NA 2
1 72 2 74 NA NA 2 11 NA 2
8 709 25 718 NA NA 2 11 NA 2
41 497 28 505 NA NA 2 12 NA 2
0.5 28 1.5 26 NA NA 2 12 NA 2
9 217 13 215 NA NA 2 12 NA 2
12 81 2 79 NA NA 2 13 NA 2
7 90 1 86 NA NA 2 13 NA 2
7 50 12 50 3 50 2 14 15 3
1.5 44 0.5 48 NA NA 3 16 NA 2
0.5 54 2.5 48 NA NA 4 16 NA 2
14 56 5 52 NA NA 5 15 NA 2
1 58 3 56 NA NA 6 7 NA 2
5 39 1 38 NA NA 7 17 NA 2
2.5 17 0.5 20 NA NA 11 12 NA 2
124 976 65 981 NA NA 11 12 NA 2
20 167 8 165 NA NA 12 18 NA 2
59 1018 43 1024 NA NA 12 19 NA 2
2 105 1 106 NA NA 12 20 NA 2
22 418 7 424 NA NA 20 21 NA 2
6 31 1 78 NA NA 20 22 NA 2
3.5 113 0.5 109 NA NA 20 22 NA 2
END
Inits
#chain 1
list(
d=c(NA,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0,0,0,0, 0,0), # one for each treatment
sd=1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,-1,-3, -2,1,1,3,-1,1,-2,-1,3,-2, -2,-3,1,-2,0,0,2,2) )
#chain 2
list(
d=c(NA,-3,1,-1,-3, -1,-3,1,-1,-3, 1,-1,-2,-3,-1, -2,-1,2,-2,3, 0,0), # one for each treatment
sd=0.1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,-1,-3, -2,1,1,3,-1,1,-2,-1,3,-2, -2,-3,1,-2,0,0,3,-2) )
#chain 3
list(
d=c(NA,0,1,1,0, 0,0,0,1,2, 3,4,2,0,0, -2,-1,2,-2,3, 0,0), # one for each treatment
sd=2,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,-1,-3, -2,1,1,3,-1,1,-2,-1,3,-2, -2,-3,1,-2,0,0,1,-1) )
M.3.6.3. WinBUGS code for inconsistency model for number of patients with DVT
# Binomial likelihood, logit link, inconsistency model
# Random effects model
model{ # *** PROGRAM STARTS
for(i in 1:ns){ # LOOP THROUGH STUDIES
delta[i,1]<-0 # treatment effect is zero in control arm
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]) { # LOOP THROUGH ARMS
r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood
logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor
#Deviance contribution
rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators
dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k]))
+ (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
# summed residual deviance contribution for this trial
resdev[i] <- sum(dev[i,1:na[i]])
for (k in 2:na[i]) { # LOOP THROUGH ARMS
# trial-specific LOR distributions
delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau)
}
}
totresdev <- sum(resdev[]) # Total Residual Deviance
for (c in 1:(nt-1)) { # priors for all mean treatment effects
for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) }
}
sd ~ dunif(0,5) # vague prior for between-trial standard deviation
var <- pow(sd,2) # between-trial variance
tau <- 1/var # between-trial precision
} # *** PROGRAM ENDS
Data
# DVT
# nt=no. treatments, ns=no. studies
list(nt=22,ns=48)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
6 24 6 28 2 29 1 2 3 3
11 48 3 49 3 48 1 2 4 3
14 51 6 46 NA NA 1 2 NA 2
11 97 11 88 NA NA 1 2 NA 2
4 118 1 108 NA NA 1 2 NA 2
12 412 4 408 NA NA 1 2 NA 2
21 50 4 48 NA NA 1 2 NA 2
17 39 3 39 NA NA 1 2 NA 2
10 50 3 50 NA NA 1 2 NA 2
20 61 10 63 NA NA 1 2 NA 2
13 33 3 31 NA NA 1 2 NA 2
4 57 6 62 NA NA 1 3 NA 2
11 97 14 97 NA NA 1 3 NA 2
17 52 5 55 NA NA 1 3 NA 2
37 103 15 97 NA NA 1 5 NA 2
6 44 2 51 NA NA 1 6 NA 2
23 47 11 48 NA NA 1 7 NA 2
4.5 93 0.5 105 NA NA 1 7 NA 2
15 33 6 33 NA NA 1 8 NA 2
11 31 2 30 NA NA 1 9 NA 2
9 41 3 39 NA NA 1 10 NA 2
14 88 4 95 NA NA 1 11 NA 2
6 107 3 101 NA NA 2 3 NA 2
1 50 9 50 NA NA 2 4 NA 2
7 429 16 431 7 430 2 11 12 3
7 190 6 195 NA NA 2 11 NA 2
5 115 5 112 NA NA 2 11 NA 2
1 72 2 74 NA NA 2 11 NA 2
8 709 25 718 NA NA 2 11 NA 2
41 497 28 505 NA NA 2 12 NA 2
0.5 28 1.5 26 NA NA 2 12 NA 2
9 217 13 215 NA NA 2 12 NA 2
12 81 2 79 NA NA 2 13 NA 2
7 90 1 86 NA NA 2 13 NA 2
7 50 12 50 3 50 2 14 15 3
1.5 44 0.5 48 NA NA 3 16 NA 2
0.5 54 2.5 48 NA NA 4 16 NA 2
14 56 5 52 NA NA 5 15 NA 2
1 58 3 56 NA NA 6 7 NA 2
5 39 1 38 NA NA 7 17 NA 2
2.5 17 0.5 20 NA NA 11 12 NA 2
124 976 65 981 NA NA 11 12 NA 2
20 167 8 165 NA NA 12 18 NA 2
59 1018 43 1024 NA NA 12 19 NA 2
2 105 1 106 NA NA 12 20 NA 2
22 418 7 424 NA NA 20 21 NA 2
6 31 1 78 NA NA 20 22 NA 2
3.5 113 0.5 109 NA NA 20 22 NA 2
END
INITS
#chain 1
list(sd=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2,1,3,1, 1,2,-3,2,-2, -2,1,0,-3,3, 0,-3,-2,-3,-2, 3,-3,0,-1,-3, 2,1,3,-2,2, 2,0,1,2,0, 0,-2,0))
# chain 2
list(sd=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0,1,3,1, 1,2,-3,2,0, 0,1,1,-3,3, 1,-3,0,-3,0, 3,-3,1,-1,-3, 2,1,3,0,2, 2,1,1,2,1, 1,0,1))
# chain 3
list(sd=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1,1,3,1, 1,2,-3,2,1, 1,1,0.5,-3,3, 0.5,-3,1,-3,1, 3,-3,0.5,-1,-3, 2,1,3,1,2, 2,0.5,1,2,0.5, 0.5,0,1))
M.3.6.4. WinBUGS code for assessment of baseline risk of PE
# Binomial likelihood, logit link # Baseline random effects model model{ # *** PROGRAM STARTS for (i in 1:ns){ # LOOP THROUGH STUDIES r[i] ~ dbin(p[i],n[i]) # Likelihood logit(p[i]) <- mu[i] # Log-odds of response mu[i] ~ dnorm(m,tau.m) # Random effects model } mu.new ~ dnorm(m,tau.m) # predictive dist. (log-odds) m ~ dnorm(0,.0001) # vague prior for mean var.m <- 1/tau.m # between-trial variance tau.m <- pow(sd.m,-2) # between-trial precision = (1/between-trial variance) sd.m ~ dunif(0,5) # vague prior for between-trial SD #tau.m ~ dgamma(0.001,0.001) #sd.m <- sqrt(var.m) logit(R) <- m # posterior probability of response logit(R.new) <- mu.new # predictive probability of response } Data list(ns=11) # ns=number of studies r[] n[] 1 97 1 52 1 24 0 50 1 17 0 97 24 54 2 61 1 41 2 88 1 47 END Inits list(mu=c(0,0,0,0,0, 0,0,0,0,0, 0), sd.m=1, m=0) list(mu = c(-1,-1,-1,-1,-1, -1,-1,-1,-1,-1, -1), sd.m=2, m= -1) list(mu = c(1,1,1,1,1, 1,1,1,1,1, 1), sd.m = 0.5, m = 1)
M.3.6.5. WinBUGS code for number of patients with PE
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
sd ~ dunif(0,5) # vague prior for random effects standard deviation
tau <- 1/pow(sd,2)
A ~ dnorm(meanA, precA) # A is on log-odds scale
precA <- pow(sdA,-2) # turn st dev into precision
for (k in 1:NT){ # v[1] will give prob of event on treat 1
logit(v[k]) <- A + d[k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
Data
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NS=26, NT=13, meanA=-3.939, sdA=2.201)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
1 97 4 97 NA NA 1 2 NA 2
1 52 2 55 NA NA 1 2 NA 2
1 24 1 29 1 28 1 2 3 3
0.5 51 2.5 49 NA NA 1 3 NA 2
1.5 18 0.5 18 NA NA 1 3 NA 2
0.5 98 4.5 89 NA NA 1 3 NA 2
24 54 9 58 NA NA 1 3 NA 2
2 61 1 63 NA NA 1 3 NA 2
1.5 42 0.5 40 NA NA 1 4 NA 2
2.5 89 0.5 96 NA NA 1 5 NA 2
1.5 48 0.5 49 NA NA 1 6 NA 2
0.5 44 1.5 48 NA NA 2 7 NA 2
0.5 71 1.5 72 NA NA 3 5 NA 2
1.5 191 0.5 196 NA NA 3 5 NA 2
11 1915 8 1894 NA NA 3 5 NA 2
1.5 73 0.5 75 NA NA 3 5 NA 2
2 429 4 431 1 430 3 5 9 3
6 90 2 86 NA NA 3 8 NA 2
4.5 498 0.5 506 NA NA 3 9 NA 2
5.5 41 0.5 41 NA NA 3 9 NA 2
0.5 469 1.5 469 NA NA 3 9 NA 2
4 976 6 981 NA NA 5 9 NA 2
1 39 1 38 NA NA 6 10 NA 2
1.5 48 0.5 54 NA NA 7 11 NA 2
2.5 168 0.5 166 NA NA 9 12 NA 2
0.5 1463 2.5 1466 NA NA 9 13 NA 2
END
Inits
#chain 1
list(
d=c(NA,0,0,0,0, 0,0,0,0,0, 0,0,0), # one for each treatment
sd=1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3) )
#chain 2
list(
d=c(NA,-3,1,-1,-3, -1,-3,1,-1,-3, 1,-1,-2), # one for each treatment
sd=0.1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3) )
#chain 3
list(
d=c(NA,0,1,1,0, 0,0,0,1,2, 3,4,2), # one for each treatment
sd=2,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3) )
M.3.6.6. WinBUGS code for inconsistency model for number of patients with PE
# Binomial likelihood, logit link, inconsistency model
# Random effects model
model{ # *** PROGRAM STARTS
for(i in 1:ns){ # LOOP THROUGH STUDIES
delta[i,1]<-0 # treatment effect is zero in control arm
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]) { # LOOP THROUGH ARMS
r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood
logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor
#Deviance contribution
rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators
dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k]))
+ (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
# summed residual deviance contribution for this trial
resdev[i] <- sum(dev[i,1:na[i]])
for (k in 2:na[i]) { # LOOP THROUGH ARMS
# trial-specific LOR distributions
delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau)
}
}
totresdev <- sum(resdev[]) # Total Residual Deviance
for (c in 1:(nt-1)) { # priors for all mean treatment effects
for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) }
}
sd ~ dunif(0,5) # vague prior for between-trial standard deviation
var <- pow(sd,2) # between-trial variance
tau <- 1/var # between-trial precision
} # *** PROGRAM ENDS
Data
# DVT
# nt=no. treatments, ns=no. studies
list(nt=13,ns=26)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
1 97 4 97 NA NA 1 2 NA 2
1 52 2 55 NA NA 1 2 NA 2
1 24 1 29 1 28 1 2 3 3
0.5 51 2.5 49 NA NA 1 3 NA 2
1.5 18 0.5 18 NA NA 1 3 NA 2
0.5 98 4.5 89 NA NA 1 3 NA 2
24 54 9 58 NA NA 1 3 NA 2
2 61 1 63 NA NA 1 3 NA 2
1.5 42 0.5 40 NA NA 1 4 NA 2
2.5 89 0.5 96 NA NA 1 5 NA 2
1.5 48 0.5 49 NA NA 1 6 NA 2
0.5 44 1.5 48 NA NA 2 7 NA 2
0.5 71 1.5 72 NA NA 3 5 NA 2
1.5 191 0.5 196 NA NA 3 5 NA 2
11 1915 8 1894 NA NA 3 5 NA 2
1.5 73 0.5 75 NA NA 3 5 NA 2
2 429 4 431 1 430 3 5 9 3
6 90 2 86 NA NA 3 8 NA 2
4.5 498 0.5 506 NA NA 3 9 NA 2
5.5 41 0.5 41 NA NA 3 9 NA 2
0.5 469 1.5 469 NA NA 3 9 NA 2
4 976 6 981 NA NA 5 9 NA 2
1 39 1 38 NA NA 6 10 NA 2
1.5 48 0.5 54 NA NA 7 11 NA 2
2.5 168 0.5 166 NA NA 9 12 NA 2
0.5 1463 2.5 1466 NA NA 9 13 NA 2
END
INITS
#chain 1
list(sd=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2,1,3,1, 1,2,-3,2,-2, -2,1,0,-3,3, 0))
# chain 2
list(sd=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0,1,3,1, 1,2,-3,2,0, 0,1,1,-3,3, 1))
# chain 3
list(sd=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1,1,3,1, 1,2,-3,2,1, 1,1,0.5,-3,3, 0.5))
M.3.6.7. WinBUGS code for assessment of baseline risk of major bleeding
# Binomial likelihood, logit link # Baseline random effects model model{ # *** PROGRAM STARTS for (i in 1:ns){ # LOOP THROUGH STUDIES r[i] ~ dbin(p[i],n[i]) # Likelihood logit(p[i]) <- mu[i] # Log-odds of response mu[i] ~ dnorm(m,tau.m) # Random effects model } mu.new ~ dnorm(m,tau.m) # predictive dist. (log-odds) m ~ dnorm(0,.0001) # vague prior for mean var.m <- 1/tau.m # between-trial variance tau.m <- pow(sd.m,-2) # between-trial precision = (1/between-trial variance) sd.m ~ dunif(0,5) # vague prior for between-trial SD #tau.m ~ dgamma(0.001,0.001) #sd.m <- sqrt(var.m) logit(R) <- m # posterior probability of response logit(R.new) <- mu.new # predictive probability of response } Data list(ns=10) # ns=number of studies r[] n[] 4 88 0 25 0 30 0 17 23 61 0 41 1 14 1 38 0 112 1 650 END Inits list(mu=c(0,0,0,0,0, 0,0,0,0,0), sd.m=1, m=0) list(mu = c(-1,-1,-1,-1,-1, -1,-1,-1,-1,-1), sd.m=2, m= -1) list(mu = c(1,1,1,1,1, 1,1,1,1,1), sd.m = 0.5, m = 1)
M.3.6.8. WinBUGS code for number of patients with major bleeding
#Random effects model for multi-arm trials (any number of arms)
model{
for(i in 1:NS){
w[i,1] <-0
delta[i,t[i,1]]<-0
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]){
r[i,k] ~ dbin(p[i,t[i,k]],n[i,k]) # binomial likelihood
logit(p[i,t[i,k]])<-mu[i] + delta[i,t[i,k]] # model
#Deviance residuals for data i
rhat[i,k] <- p[i,t[i,k]] * n[i,k] dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k])) + (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
sdev[i]<- sum(dev[i,1:na[i]])
for (k in 2:na[i]){
# trial-specific LOR distributions
delta[i,t[i,k]] ~ dnorm(md[i,t[i,k]],taud[i,t[i,k]])
md[i,t[i,k]] <- d[t[i,k]] - d[t[i,1]] + sw[i,k] # mean of LOR distributions
taud[i,t[i,k]] <- tau *2*(k-1)/k #precision of LOR distributions
#adjustment, multi-arm RCTs
w[i,k] <- (delta[i,t[i,k]] - d[t[i,k]] + d[t[i,1]])
# cumulative adjustment for multi-arm trials
sw[i,k] <-sum(w[i,1:k-1])/(k-1)
}
}
d[1]<-0
for (k in 2:NT){d[k] ~ dnorm(0,.0001) } # vague priors for basic parameters
sd ~ dunif(0,5) # vague prior for random effects standard deviation
tau <- 1/pow(sd,2)
A ~ dnorm(meanA, precA) # A is on log-odds scale
precA <- pow(sdA,-2) # turn st dev into precision
for (k in 1:NT){ # v[1] will give prob of event on treat 1
logit(v[k]) <- A + d[k]
rr[k] <- v[k]/v[1] # calculate relative risk
}
sumdev <- sum(sdev[]) # Calculate residual deviance
# Ranking and prob{treatment k is best}
for (k in 1:NT){
rk[k] <- rank(rr[],k)
best[k] <- equals(rank(rr[],k),1)
}
# pairwise ORs and RRs
for (c in 1:(NT-1)){
for (k in (c+1):NT){
lor[c,k] <- d[k] - d[c]
log(or[c,k]) <- lor[c,k]
lrr[c,k] <- log(rr[k]) - log(rr[c])
log(rrisk[c,k]) <- lrr[c,k]
}
}
}
Data
# NT=no. treatments, NS=no. studies;
# NB : set up M vectors each r[,]. n[,] and t[,], where M is the Maximum number of treatments
# per trial in the dataset. In this dataset M is 3.
list(NS=29, NT=8, meanA=-5.331 sdA=3.482)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
4 88 4 95 NA NA 1 2 NA 2
0.5 26 0.5 26 1.5 26 1 3 4 3
0.5 31 6.5 31 NA NA 1 3 NA 2
0.5 18 1.5 18 NA NA 1 3 NA 2
23 61 24 63 NA NA 1 3 NA 2
0.5 42 1.5 40 NA NA 1 4 NA 2
1 14 2 16 NA NA 1 4 NA 2
1 38 5 109 NA NA 1 4 NA 2
0.5 113 2.5 109 NA NA 1 4 NA 2
1 650 10 635 NA NA 1 5 NA 2
14 71 9 70 NA NA 2 3 NA 2
0.5 38 6.5 32 NA NA 2 3 NA 2
69 1894 91 1915 NA NA 2 3 NA 2
17 74 23 72 NA NA 2 3 NA 2
14 431 12 429 10 430 2 3 6 3
2 112 15 115 NA NA 2 3 NA 2
11 725 18 719 NA NA 2 3 NA 2
3 1034 13 1036 NA NA 2 6 NA 2
0.5 17 1.5 20 NA NA 2 6 NA 2
2 217 10 215 NA NA 3 6 NA 2
13 110 32 105 NA NA 3 6 NA 2
1 40 2 40 NA NA 3 6 NA 2
5.5 83 0.5 85 NA NA 3 6 NA 2
10 643 18 653 NA NA 3 6 NA 2
1 27 1 25 NA NA 3 6 NA 2
1 20 6 23 NA NA 3 7 NA 2
49 1433 34 1425 NA NA 5 6 NA 2
1 248 3 253 NA NA 6 8 NA 2
4 222 1 205 NA NA 6 8 NA 2
END
Inits
#chain 1
list(
d=c(NA,0,0,0,0, 0,0,0), # one for each treatment
sd=1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,1) )
#chain 2
list(
d=c(NA,-3,1,-1,-3, -1,-3,1), # one for each treatment
sd=0.1,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,3) )
#chain 3
list(
d=c(NA,0,1,1,0, 0,0,0), # one for each treatment
sd=2,
mu=c(3,2,-3,1,0,3,-2,-1,2,-2, -1,3,1,3,-2,-1,2,-2,3,-1, 1,-1,-2,-3,-1,-3,0,2,0) )
M.3.6.9. WinBUGS code for inconsistency model for number of patients with major bleeding
# Binomial likelihood, logit link, inconsistency model
# Random effects model
model{ # *** PROGRAM STARTS
for(i in 1:ns){ # LOOP THROUGH STUDIES
delta[i,1]<-0 # treatment effect is zero in control arm
mu[i] ~ dnorm(0,.0001) # vague priors for trial baselines
for (k in 1:na[i]) { # LOOP THROUGH ARMS
r[i,k] ~ dbin(p[i,k],n[i,k]) # binomial likelihood
logit(p[i,k]) <- mu[i] + delta[i,k] # model for linear predictor
#Deviance contribution
rhat[i,k] <- p[i,k] * n[i,k] # expected value of the numerators
dev[i,k] <- 2 * (r[i,k] * (log(r[i,k])-log(rhat[i,k]))
+ (n[i,k]-r[i,k]) * (log(n[i,k]-r[i,k]) - log(n[i,k]-rhat[i,k])))
}
# summed residual deviance contribution for this trial
resdev[i] <- sum(dev[i,1:na[i]])
for (k in 2:na[i]) { # LOOP THROUGH ARMS
# trial-specific LOR distributions
delta[i,k] ~ dnorm(d[t[i,1],t[i,k]] ,tau)
}
}
totresdev <- sum(resdev[]) # Total Residual Deviance
for (c in 1:(nt-1)) { # priors for all mean treatment effects
for (k in (c+1):nt) { d[c,k] ~ dnorm(0,.0001) }
}
sd ~ dunif(0,5) # vague prior for between-trial standard deviation
var <- pow(sd,2) # between-trial variance
tau <- 1/var # between-trial precision
} # *** PROGRAM ENDS
Data
# Major bleeding
# nt=no. treatments, ns=no. studies
list(nt=8,ns=29)
r[,1] n[,1] r[,2] n[,2] r[,3] n[,3] t[,1] t[,2] t[,3] na[]
4 88 4 95 NA NA 1 2 NA 2
0.5 26 0.5 26 1.5 26 1 3 4 3
0.5 31 6.5 31 NA NA 1 3 NA 2
0.5 18 1.5 18 NA NA 1 3 NA 2
23 61 24 63 NA NA 1 3 NA 2
0.5 42 1.5 40 NA NA 1 4 NA 2
1 14 2 16 NA NA 1 4 NA 2
1 38 5 109 NA NA 1 4 NA 2
0.5 113 2.5 109 NA NA 1 4 NA 2
1 650 10 635 NA NA 1 5 NA 2
14 71 9 70 NA NA 2 3 NA 2
0.5 38 6.5 32 NA NA 2 3 NA 2
69 1894 91 1915 NA NA 2 3 NA 2
17 74 23 72 NA NA 2 3 NA 2
14 431 12 429 10 430 2 3 6 3
2 112 15 115 NA NA 2 3 NA 2
11 725 18 719 NA NA 2 3 NA 2
3 1034 13 1036 NA NA 2 6 NA 2
0.5 17 1.5 20 NA NA 2 6 NA 2
2 217 10 215 NA NA 3 6 NA 2
13 110 32 105 NA NA 3 6 NA 2
1 40 2 40 NA NA 3 6 NA 2
5.5 83 0.5 85 NA NA 3 6 NA 2
10 643 18 653 NA NA 3 6 NA 2
1 27 1 25 NA NA 3 6 NA 2
1 20 6 23 NA NA 3 7 NA 2
49 1433 34 1425 NA NA 5 6 NA 2
1 248 3 253 NA NA 6 8 NA 2
4 222 1 205 NA NA 6 8 NA 2
END
INITS
#chain 1
list(sd=1, mu=c(2,0,3,0,2, -2,2,-2,-1,3, 2,-2,1,3,1, 1,2,-3,2,-2, -2,1,0,-3,3, 0,-3,-2,-3))
# chain 2
list(sd=1.5, mu=c(2,1,3,1,2, 0,2,0,-1,3, 2,0,1,3,1, 1,2,-3,2,0, 0,1,1,-3,3, 1,-3,0,-3))
# chain 3
list(sd=3, mu=c(2,0.5,3,0.5,2, -2,2,1,-1,3, 2,1,1,3,1, 1,2,-3,2,1, 1,1,0.5,-3,3, 0.5,-3,1,-3))
- Network meta-analyses (NMAs) - Venous thromboembolism in over 16sNetwork meta-analyses (NMAs) - Venous thromboembolism in over 16s
Your browsing activity is empty.
Activity recording is turned off.
See more...